


-
 Alergia
Alergia -
 Anestesiología
Anestesiología -
 Bioquímica
Bioquímica
-
 Cardiología
Cardiología
-
 Cirugía
Cirugía
-
 Dermatología
Dermatología
-
 Endocrinología y Metabolismo
Endocrinología y Metabolismo
-
 Enfermería
Enfermería
-
 Gastroenterología
Gastroenterología
-
 Hematología
Hematología
-
 Infectología
Infectología
-
 Inmunología
Inmunología
-
 Medicina Interna
Medicina Interna
-
 Nefrología
Nefrología
-
 Neumonología
Neumonología
-
 Neurología
Neurología
-
 Nutrición
Nutrición
-
 Obstetricia y Ginecología
Obstetricia y Ginecología
-
 Odontología
Odontología
-
 Oncología
Oncología
-
 Otorrinolaringología
Otorrinolaringología
-
 Pediatría
Pediatría
-
 Salud Mental
Salud Mental
-
 Salud Pública
Salud Pública
-
 Urología
Urología
-
 Más Especialidades
Más Especialidades
- Índice
-
Acceso por especialidad
-
Alergia
-
Anestesiología
-
Bioquímica
-
Cardiología
-
Cirugía
-
Dermatología
-
Endocrinología y Metabolismo
-
Enfermería
-
Gastroenterología
-
Hematología
-
Infectología
-
Inmunología
-
Medicina Interna
-
Nefrología
-
Neumonología
-
Neurología
-
Nutrición
-
Obstetricia y Ginecología
-
Odontología
-
Oncología
-
Otorrinolaringología
-
Pediatría
-
Salud Mental
-
Salud Pública
-
Urología
-
Más Especialidades
-
Noticias biomédicas

-
Fuentes informativas
- Editoriales
-
COVID-19
-
INFORMES CIENTÍFICOS
- Preguntas con Respuesta
- América Latina Investiga
- Completos revisados (full text)
-
NOTICIAS/OPINIONES
-
Expertos invitados
- Por especialidad
- de Iberoamérica
- del mundo
- Entrevistas
- Casos clínicos
-
Crónicas de Autores
- Authors’ Reports
-
Instrucciones para autores
-
Expertos Preguntan
-
Novedades
- ViASIIC
- Medicina del Dolor
-
Por especialidad
-
Iberomédica
-
Informes comentados
- Textos Completos Autorizados
- Preocupaciones Profesionales
-
Red Científica Iberoamericana (RedCIbe)
-
Conceptos Categoricos
-
Acceso por especialidad

-
Alergia
-
Anestesiología
-
Bioquímica
-
Cardiología
-
Cirugía
-
Dermatología
-
Endocrinología y Metabolismo
-
Enfermería
-
Gastroenterología
-
Hematología
-
Infectología
-
Inmunología
-
Medicina Interna
-
Nefrología
-
Neumonología
-
Neurología
-
Nutrición
-
Obstetricia y Ginecología
-
Odontología
-
Oncología
-
Otorrinolaringología
-
Pediatría
-
Salud Mental
-
Salud Pública
-
Urología
-
Más Especialidades
-
Noticias biomédicas
-
Fuentes informativas
- Editoriales
- Covid-19
-
Informes Científicos
- Preguntas con Respuesta
- América Latina Investiga
- Completos revisados (full text)
- Noticias/Opiniones
- Noticias (castellano/portugués)
- Noticias (otros idiomas)
- Expertos invitados
- Por especialidad
- de Iberoamérica
- del mundo
- Entrevistas
- Casos clínicos
-
Crónicas de Autores
- Authors’ Reports
-
Instrucciones para autores
-
Expertos Preguntan
- Novedades
- ViASIIC
- Medicina del Dolor
-
Por especialidad
-
Iberomédica
-
Informes comentados
- Textos Completos Autorizados
- Preocupaciones Profesionales
- Red Científica Iberoamericana
- Por materia
- Por fecha
-
Conceptos Categóricos

Casos Clínicos
TRATAMIENTO QUIRURGICO EFECTIVO DEL GRANULOMA DE CELULAS GIGANTES DEL MAXILAR SUPERIOR
Si bien es una lesión benigna, el granuloma central de células gigantes puede provocar erosión ósea y asimetría facial. Se describe el tratamiento quirúrgico exitoso de una lesión de estas características ubicada en el maxilar superior.
Coautores
Seyyed Mohammad Homauni*
Assistant Professor of Internal Medicine, Shahid Beheshti University of Medical Sciences, Teherán, Irán*
Seyyed Mohammad Homauni*
Assistant Professor of Internal Medicine, Shahid Beheshti University of Medical Sciences, Teherán, Irán*
Clasificación en siicsalud
Artículos originales > Expertos del Mundo >
página /dato/casiic.php/106590
Especialidades

Artículos originales > Expertos del Mundo >
página /dato/casiic.php/106590
Especialidades
Primera edición en siicsalud
26 de enero, 2010
26 de enero, 2010
TRATAMIENTO QUIRURGICO EFECTIVO DEL GRANULOMA DE CELULAS GIGANTES DEL MAXILAR SUPERIOR
(especial para SIIC © Derechos reservados)
(especial para SIIC © Derechos reservados)
Introducción
Jaffe suponía que las lesiones mandibulares no eran verdaderas neoplasias y que representaban reacciones locales reparativas.1,2 Debido a que el comportamiento clínico de muchas de estas lesiones no es compatible con un proceso de reparación, el término “reparativo” se ha omitido en la actualidad.3,4 Si bien algunas lesiones presentan un comportamiento agresivo semejante al de una neoplasia, actualmente estos procesos se designan como granulomas de células gigantes o con el nombre menos restrictivo de lesiones de células gigantes. Es aún motivo de controversia si existen verdaderos tumores de células gigantes en los maxilares.5 El granuloma central de células gigantes (GCCG) de los maxilares es una lesión benigna.1,3 La OMS define el GCCG como una lesión intraósea conformada por tejido celular fibroso que contiene numerosos focos de hemorragia, agregados de células gigantes multinucleares y, ocasionalmente, de trabéculas de hueso reticulado.6
Los GCCG de los maxilares se observan principalmente en niños y en adultos jóvenes, en especial en mujeres. Son más comunes en la mandíbula que en el maxilar superior y pueden estar confinados a las arcadas dentarias de los maxilares.1 Los GCCG pueden afectar también los huesos extramaxilares, sobre todo en la región craneofacial.7,8 Existe considerable variación en el comportamiento clínico de los GCCG. Pueden aparecer con rápido inicio de dolor, parestesias, reabsorción de raíces y desplazamiento dentario. Esta forma de presentación puede expandirse o destruir el hueso que la rodea, lo que resulta en asimetría facial. Otras formas de GCCG son en ocasiones asintomáticas y pueden verse simplemente en una evaluación dental de rutina.9-11
El raspado quirúrgico minucioso es aún el tratamiento de elección. Las lesiones recurrentes a menudo responden a una nueva cirugía, aunque algunas lesiones agresivas y aquellas con numerosas recurrencias pueden requerir una cirugía más radical o interferón alfa.5
Caso clínico
Una mujer de 26 años fue derivada a nuestra clínica por tumefacción en el área del maxilar superior derecho que ella interpretó inicialmente como un quiste odontógeno. Señaló que la había advertido varios meses atrás, cuando comenzó la tumefacción en el rostro.
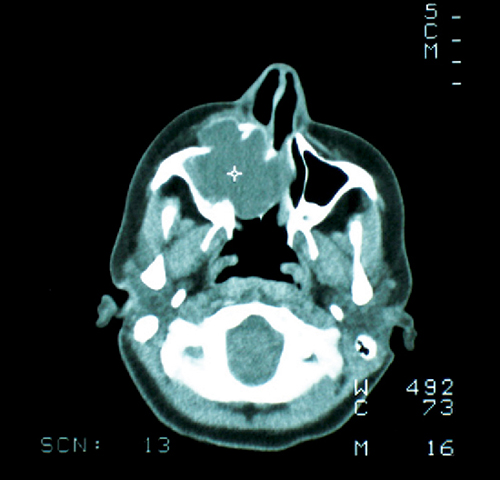
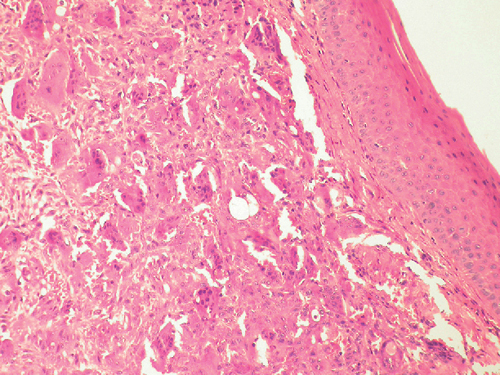
En la evaluación de la cavidad oral se observó que los molares del maxilar superior derecho se encontraban móviles, con firme tumefacción por encima de las raíces a nivel bucal y palatino. El examen físico, por lo demás, resultó normal. Las pruebas de laboratorio fueron normales, incluidos los niveles de calcio, fósforo y fosfatasa alcalina. Las radiografías no son muy útiles; las imágenes por tomografía computarizada definieron mejor la extensión de la lesión hacia el seno, representada por la perforación del maxilar superior y el malar (Figura 1). Se tomó una biopsia de la lesión a través de la cavidad oral bajo anestesia local. El informe histopatológico (Figura 2) confirmó el diagnóstico de GCCG.
Antes de la cirugía se fabricó un implante maxilar que incluía piezas dentarias. Bajo anestesia general, se efectuó una incisión parcial extrabucal de Weber-Ferguson para acceder a la lesión. Se expusieron los planos intraorales, bucal y palatino. Luego, se extrajeron los dientes del hemimaxilar superior derecho y después se resecó la lesión mediante raspado quirúrgico. Por debajo del piso de la órbita, la mucosa del seno maxilar se encontraba comprimida por la lesión en dirección cefálica. No se requirieron injertos. Se suturaron las heridas con poligactina y se insertó la prótesis intraoral. La paciente recibió dos unidades de sangre durante la cirugía debido a la hemorragia profusa durante el procedimiento. La hemorragia se detuvo después de la resección completa de la lesión. No se observaron eventos en la paciente en el período posoperatorio y la evolución es buena después de 15 años de la cirugía, sin recurrencias.
Muchos autores todavía recomiendan firmemente el tratamiento de los CGGC mediante la exéresis quirúrgica.11 La extensión de la cirugía depende del tamaño y la localización de la lesión, así como de su evolución; puede variar de la simple exéresis con raspado quirúrgico a la resección en bloque.9 Las lesiones agresivas de células gigantes han sido tratadas también con otros métodos, como la radiación, la administración sistémica de calcitonina, las inyecciones intralesionales de corticoides, la aplicación subcutánea de interferón alfa y el tratamiento con láser, incluido el láser de dióxido de carbono.10,11 En nuestro caso, la exéresis quirúrgica y el raspado del hueso remanente fueron curativos.
Algunos CGGC de los maxilares, a pesar de la presentación típica clínica, histológica y radiológica, se caracterizan por una conducta agresiva y tienden a la recurrencia. Ficarra y col. 12 consideraron que estas lesiones deberían definirse como CGGC agresivos de los maxilares; además se ha descrito la recurrencia después del raspado quirúrgico. Es altamente probable que estos subtipos tengan una misma naturaleza y que sus diferencias en el comportamiento biológico se deban a las distintas condiciones subyacentes entre los pacientes.
Los autores no manifiestan conflictos de intereses.
Jaffe suponía que las lesiones mandibulares no eran verdaderas neoplasias y que representaban reacciones locales reparativas.1,2 Debido a que el comportamiento clínico de muchas de estas lesiones no es compatible con un proceso de reparación, el término “reparativo” se ha omitido en la actualidad.3,4 Si bien algunas lesiones presentan un comportamiento agresivo semejante al de una neoplasia, actualmente estos procesos se designan como granulomas de células gigantes o con el nombre menos restrictivo de lesiones de células gigantes. Es aún motivo de controversia si existen verdaderos tumores de células gigantes en los maxilares.5 El granuloma central de células gigantes (GCCG) de los maxilares es una lesión benigna.1,3 La OMS define el GCCG como una lesión intraósea conformada por tejido celular fibroso que contiene numerosos focos de hemorragia, agregados de células gigantes multinucleares y, ocasionalmente, de trabéculas de hueso reticulado.6
Los GCCG de los maxilares se observan principalmente en niños y en adultos jóvenes, en especial en mujeres. Son más comunes en la mandíbula que en el maxilar superior y pueden estar confinados a las arcadas dentarias de los maxilares.1 Los GCCG pueden afectar también los huesos extramaxilares, sobre todo en la región craneofacial.7,8 Existe considerable variación en el comportamiento clínico de los GCCG. Pueden aparecer con rápido inicio de dolor, parestesias, reabsorción de raíces y desplazamiento dentario. Esta forma de presentación puede expandirse o destruir el hueso que la rodea, lo que resulta en asimetría facial. Otras formas de GCCG son en ocasiones asintomáticas y pueden verse simplemente en una evaluación dental de rutina.9-11
El raspado quirúrgico minucioso es aún el tratamiento de elección. Las lesiones recurrentes a menudo responden a una nueva cirugía, aunque algunas lesiones agresivas y aquellas con numerosas recurrencias pueden requerir una cirugía más radical o interferón alfa.5
Caso clínico
Una mujer de 26 años fue derivada a nuestra clínica por tumefacción en el área del maxilar superior derecho que ella interpretó inicialmente como un quiste odontógeno. Señaló que la había advertido varios meses atrás, cuando comenzó la tumefacción en el rostro.
En la evaluación de la cavidad oral se observó que los molares del maxilar superior derecho se encontraban móviles, con firme tumefacción por encima de las raíces a nivel bucal y palatino. El examen físico, por lo demás, resultó normal. Las pruebas de laboratorio fueron normales, incluidos los niveles de calcio, fósforo y fosfatasa alcalina. Las radiografías no son muy útiles; las imágenes por tomografía computarizada definieron mejor la extensión de la lesión hacia el seno, representada por la perforación del maxilar superior y el malar (Figura 1). Se tomó una biopsia de la lesión a través de la cavidad oral bajo anestesia local. El informe histopatológico (Figura 2) confirmó el diagnóstico de GCCG.
Antes de la cirugía se fabricó un implante maxilar que incluía piezas dentarias. Bajo anestesia general, se efectuó una incisión parcial extrabucal de Weber-Ferguson para acceder a la lesión. Se expusieron los planos intraorales, bucal y palatino. Luego, se extrajeron los dientes del hemimaxilar superior derecho y después se resecó la lesión mediante raspado quirúrgico. Por debajo del piso de la órbita, la mucosa del seno maxilar se encontraba comprimida por la lesión en dirección cefálica. No se requirieron injertos. Se suturaron las heridas con poligactina y se insertó la prótesis intraoral. La paciente recibió dos unidades de sangre durante la cirugía debido a la hemorragia profusa durante el procedimiento. La hemorragia se detuvo después de la resección completa de la lesión. No se observaron eventos en la paciente en el período posoperatorio y la evolución es buena después de 15 años de la cirugía, sin recurrencias.
Figura 1. Tomografía axial computarizada en la que se observa el tumor y la destrucción de las paredes lateral y medial del seno maxilar.
Figura 2. Microfotografía de mediano aumento en la que se observan numerosas células gigantes en un estroma celular fibroso (tinción con hematoxilina y eosina).Discusión
Muchos autores todavía recomiendan firmemente el tratamiento de los CGGC mediante la exéresis quirúrgica.11 La extensión de la cirugía depende del tamaño y la localización de la lesión, así como de su evolución; puede variar de la simple exéresis con raspado quirúrgico a la resección en bloque.9 Las lesiones agresivas de células gigantes han sido tratadas también con otros métodos, como la radiación, la administración sistémica de calcitonina, las inyecciones intralesionales de corticoides, la aplicación subcutánea de interferón alfa y el tratamiento con láser, incluido el láser de dióxido de carbono.10,11 En nuestro caso, la exéresis quirúrgica y el raspado del hueso remanente fueron curativos.
Algunos CGGC de los maxilares, a pesar de la presentación típica clínica, histológica y radiológica, se caracterizan por una conducta agresiva y tienden a la recurrencia. Ficarra y col. 12 consideraron que estas lesiones deberían definirse como CGGC agresivos de los maxilares; además se ha descrito la recurrencia después del raspado quirúrgico. Es altamente probable que estos subtipos tengan una misma naturaleza y que sus diferencias en el comportamiento biológico se deban a las distintas condiciones subyacentes entre los pacientes.
Los autores no manifiestan conflictos de intereses.
Surgical Management of an Aggressive Central Giant Cell Granuloma of the Maxilla
(especial para SIIC © Derechos reservados)
(especial para SIIC © Derechos reservados)
Introduction
Jaffe believed that jaw lesions were not true neoplasms and that they represented a local reparative reaction.1,2 Because the clinical behavior of many of these lesions is inconsistent with a reparative process, the term “reparative” has been omitted today.3,4 Although some lesions demonstrate aggressive behavior similar to that of a neoplasm, today these lesions are designated giant cell granuloma or by the more noncommittal name of giant cell lesion. Whether or not true giant cell tumors occur in the jaws is still controversial.5 Central giant cell granuloma (CGCG) of the jaws is a benign lesion.1,3 Central GCG is defined by the World Health Organization as an intraosseous lesion consisting of cellular fibrous tissue containing multiple foci of hemorrhage, aggregations of multinucleated giant cells, and, occasionally, trabeculae of woven bone.6 Central GCGs of the jaws mainly occur in children or in young adults, especially in females. It is more common in the mandible than in the maxilla and can be confined to the tooth-bearing areas of the jaws.1 CGCG can also affect extragnathic bones, mainly in the craniofacial region.7,8 There is considerable variation in the clinical behavior of CGCG. It may occur with a rapid onset of pain, paresthesia, root resorption, and tooth displacement. This form is also able to expand or destroy surrounding bone, resulting in facial asymmetry. Another form of CGCG is sometimes asymptomatic and may be seen simply through routine dental examinations.9-11 Thorough curettage is still the treatment of choice for this lesion. Recurrent lesions often respond to further curettage, although some aggressive lesions and those with multiple recurrences may require more radical surgery or alpha interferon.5
Case report
A 26-year-old female was referred to our clinic for a swelling in the area of the right maxilla which she initially thought to be an odontogenic cyst. She stated that she had noticed it several months ago when her face had started to swell. Intraoral examination showed the right maxillary molars to be mobile with firm swelling above the roots buccally and in the palate. Physical examination was otherwise normal. Laboratory tests including calcium and phosphorous and alkaline phosphatase levels were normal. Radiographs were not very helpful; CT scans better defined the extent of the lesion within the antrum depicting perforation of the maxilla and zygoma (Figure 1). A biopsy was taken from the lesion intraorally under local anesthesia. The pathology report (Figure 2) confirmed the diagnosis of a CGCG. A maxillary splint which included teeth was fabricated prior to surgery. Under general anesthesia, a partial Weber-Ferguson extraoral incision was made to access the lesion. Intraorally, buccal and palatal flaps were raised. Then, the teeth of the right hemimaxilla were removed; next, the lesion was removed via curettage. Below the orbital floor, the sinus mucosa was compressed upward by the lesion. No grafts were necessary. The wounds were sutured with polygalactin sutures and the intraoral splint was placed. The patient received 2 units of blood during the operation for profuse bleeding throughout the operation. Oozing stopped after complete removal of the lesion. The patient's postoperative course was uneventful and the she is doing well 15 years postoperatively without recurrence.
Treatment of CGCG by surgical excision is still strongly supported by many authors.11 The extent of surgery depends upon the size and site of the lesion, as well as its course; it may range from simple excision and curettage to en bloc resection.9 Aggressive giant cell lesions have also been treated with other methods such as radiation, systemic application of calcitonin, intralesional injections of corticosteroids, and subcutaneous alpha-interferon injections and laser therapy, including carbon dioxide laser.10,11 In our case, surgical excision and curettage of remaining bone was curative.
Some CGCGs of the jaws, despite a typical histological, radiological, and clinical presentation, show aggressive behavior and tend to recur. Ficarra et al.12 considered that these lesions should be defined as aggressive CGCG of the jaws, and recurrence following curettage has been reported. It is highly probable that these subtypes are the same in nature and their different biologic behavior reflect different underlying conditions among patients.
Jaffe believed that jaw lesions were not true neoplasms and that they represented a local reparative reaction.1,2 Because the clinical behavior of many of these lesions is inconsistent with a reparative process, the term “reparative” has been omitted today.3,4 Although some lesions demonstrate aggressive behavior similar to that of a neoplasm, today these lesions are designated giant cell granuloma or by the more noncommittal name of giant cell lesion. Whether or not true giant cell tumors occur in the jaws is still controversial.5 Central giant cell granuloma (CGCG) of the jaws is a benign lesion.1,3 Central GCG is defined by the World Health Organization as an intraosseous lesion consisting of cellular fibrous tissue containing multiple foci of hemorrhage, aggregations of multinucleated giant cells, and, occasionally, trabeculae of woven bone.6 Central GCGs of the jaws mainly occur in children or in young adults, especially in females. It is more common in the mandible than in the maxilla and can be confined to the tooth-bearing areas of the jaws.1 CGCG can also affect extragnathic bones, mainly in the craniofacial region.7,8 There is considerable variation in the clinical behavior of CGCG. It may occur with a rapid onset of pain, paresthesia, root resorption, and tooth displacement. This form is also able to expand or destroy surrounding bone, resulting in facial asymmetry. Another form of CGCG is sometimes asymptomatic and may be seen simply through routine dental examinations.9-11 Thorough curettage is still the treatment of choice for this lesion. Recurrent lesions often respond to further curettage, although some aggressive lesions and those with multiple recurrences may require more radical surgery or alpha interferon.5
Case report
A 26-year-old female was referred to our clinic for a swelling in the area of the right maxilla which she initially thought to be an odontogenic cyst. She stated that she had noticed it several months ago when her face had started to swell. Intraoral examination showed the right maxillary molars to be mobile with firm swelling above the roots buccally and in the palate. Physical examination was otherwise normal. Laboratory tests including calcium and phosphorous and alkaline phosphatase levels were normal. Radiographs were not very helpful; CT scans better defined the extent of the lesion within the antrum depicting perforation of the maxilla and zygoma (Figure 1). A biopsy was taken from the lesion intraorally under local anesthesia. The pathology report (Figure 2) confirmed the diagnosis of a CGCG. A maxillary splint which included teeth was fabricated prior to surgery. Under general anesthesia, a partial Weber-Ferguson extraoral incision was made to access the lesion. Intraorally, buccal and palatal flaps were raised. Then, the teeth of the right hemimaxilla were removed; next, the lesion was removed via curettage. Below the orbital floor, the sinus mucosa was compressed upward by the lesion. No grafts were necessary. The wounds were sutured with polygalactin sutures and the intraoral splint was placed. The patient received 2 units of blood during the operation for profuse bleeding throughout the operation. Oozing stopped after complete removal of the lesion. The patient's postoperative course was uneventful and the she is doing well 15 years postoperatively without recurrence.
Figure 1. Axial CT scan depicting the tumor and destruction of the lateral and medial walls of the antrum.
Figure 2. Medium power micrograph showing numerous giant cells in a cellular fibrous stroma (H&E).Discussion
Treatment of CGCG by surgical excision is still strongly supported by many authors.11 The extent of surgery depends upon the size and site of the lesion, as well as its course; it may range from simple excision and curettage to en bloc resection.9 Aggressive giant cell lesions have also been treated with other methods such as radiation, systemic application of calcitonin, intralesional injections of corticosteroids, and subcutaneous alpha-interferon injections and laser therapy, including carbon dioxide laser.10,11 In our case, surgical excision and curettage of remaining bone was curative.
Some CGCGs of the jaws, despite a typical histological, radiological, and clinical presentation, show aggressive behavior and tend to recur. Ficarra et al.12 considered that these lesions should be defined as aggressive CGCG of the jaws, and recurrence following curettage has been reported. It is highly probable that these subtypes are the same in nature and their different biologic behavior reflect different underlying conditions among patients.
Mohammad Hosein Motamedi, Baqiyatallah University of Medical Sciences Trauma Research Center, 19667, Teherán, Irán,
e-mail: motamedical@lycos.com
1. Kruse-Losler B, Diallo R, Gaertner C, Mischke KL, Joos U, Kleinheinz J. Central giant cell granuloma of the jaws: a clinical, radiologic, and histopathologic study of 26 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101:346-54, 2006.
2. Jaffe HL. Giant cell reparative granuloma, traumatic bone cyst and fibrous (fibro-osseous) dysplasia of jaw bones. Oral Surg 6:159-75, 1953.
3. Regezi JA, Sciubba JJ. Oral Pathology. St. Louis: Saunders pp. 116-7, 298-301, 2003.
4. De Lange J, Van den Akker HP. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 99:464-70, 2005.
5. Neville BW, Damm DD, Allen CM, Bouquo JE. Oral and maxillofacial pathology. Philadelphia, Saunders pp. 449-51, 544-7, 2002.
6. Kramer IRH, Pindborg JJ, Shear M, editors. Histological typing of odontogenic tumours. 2nd ed. Berlin, Springer-Verlag p. 31, 1991.
7. Yamaguchi T, Dorfman HD. Giant cell reparative granuloma: a comparative clinicopathologic study of lesions in gnathic and extragnathic sites. Int J Surg Pathol 9:189-200, 2001.
8. Boedeker CC, Kayser G, Ridder GJ, Maier W, Schipper J. Giant cell reparative granuloma of the temporal bone: a case report and review of the literature. Ear Nose Throat J 82:926-37, 2003.
9. Farrier SL, Farrier JN, Smart MK, Nash ES. A 10-year review of the occurrence and treatment of central giant cell granulomas, in a District General Hospital. J Oral Pathol Med 35:332-7, 2006.
10. Chaparro Avendano AV, Berini Aytes L, Gay Escoda C. Peripheral giant cell granuloma. A report of five cases and review of the literature. Med Oral Patol Oral Cir Bucal 10:53-7, 2005.
11. Motamedi MH, Eshghyar N, Jafari SM, Lassemi E, Navi F, Abbas FM, Khalifeh S, Eshkevari PS. Peripheral and central giant cell granulomas of the jaws: a demographic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 103(6):e39-43, 2007. Epub 2007 Apr 11.
12. Ficarra G, Kaban LB, Hansen LS. Central giant cell lesions of the mandible and maxilla: a clinicopathologic and cytometric study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 64:44-9, 1987.
Está expresamente prohibida la redistribución y la redifusión de todo o parte de los
contenidos de la Sociedad Iberoamericana de Información Científica (SIIC) S.A. sin
previo y expreso consentimiento de SIIC.
ua91218

