


-
 Alergia
Alergia -
 Anestesiología
Anestesiología -
 Bioquímica
Bioquímica
-
 Cardiología
Cardiología
-
 Cirugía
Cirugía
-
 Dermatología
Dermatología
-
 Endocrinología y Metabolismo
Endocrinología y Metabolismo
-
 Enfermería
Enfermería
-
 Gastroenterología
Gastroenterología
-
 Hematología
Hematología
-
 Infectología
Infectología
-
 Inmunología
Inmunología
-
 Medicina Interna
Medicina Interna
-
 Nefrología
Nefrología
-
 Neumonología
Neumonología
-
 Neurología
Neurología
-
 Nutrición
Nutrición
-
 Obstetricia y Ginecología
Obstetricia y Ginecología
-
 Odontología
Odontología
-
 Oncología
Oncología
-
 Otorrinolaringología
Otorrinolaringología
-
 Pediatría
Pediatría
-
 Salud Mental
Salud Mental
-
 Salud Pública
Salud Pública
-
 Urología
Urología
-
 Más Especialidades
Más Especialidades
- Índice
-
Acceso por especialidad
-
Alergia
-
Anestesiología
-
Bioquímica
-
Cardiología
-
Cirugía
-
Dermatología
-
Endocrinología y Metabolismo
-
Enfermería
-
Gastroenterología
-
Hematología
-
Infectología
-
Inmunología
-
Medicina Interna
-
Nefrología
-
Neumonología
-
Neurología
-
Nutrición
-
Obstetricia y Ginecología
-
Odontología
-
Oncología
-
Otorrinolaringología
-
Pediatría
-
Salud Mental
-
Salud Pública
-
Urología
-
Más Especialidades
-
Noticias biomédicas

-
Fuentes informativas
- Editoriales
-
COVID-19
-
INFORMES CIENTÍFICOS
- Preguntas con Respuesta
- América Latina Investiga
- Completos revisados (full text)
-
NOTICIAS/OPINIONES
-
Expertos invitados
- Por especialidad
- de Iberoamérica
- del mundo
- Entrevistas
- Casos clínicos
-
Crónicas de Autores
- Authors’ Reports
-
Instrucciones para autores
-
Expertos Preguntan
-
Novedades
- ViASIIC
- Medicina del Dolor
-
Por especialidad
-
Iberomédica
-
Informes comentados
- Textos Completos Autorizados
- Preocupaciones Profesionales
-
Red Científica Iberoamericana (RedCIbe)
-
Conceptos Categoricos
-
Acceso por especialidad

-
Alergia
-
Anestesiología
-
Bioquímica
-
Cardiología
-
Cirugía
-
Dermatología
-
Endocrinología y Metabolismo
-
Enfermería
-
Gastroenterología
-
Hematología
-
Infectología
-
Inmunología
-
Medicina Interna
-
Nefrología
-
Neumonología
-
Neurología
-
Nutrición
-
Obstetricia y Ginecología
-
Odontología
-
Oncología
-
Otorrinolaringología
-
Pediatría
-
Salud Mental
-
Salud Pública
-
Urología
-
Más Especialidades
-
Noticias biomédicas
-
Fuentes informativas
- Editoriales
- Covid-19
-
Informes Científicos
- Preguntas con Respuesta
- América Latina Investiga
- Completos revisados (full text)
- Noticias/Opiniones
- Noticias (castellano/portugués)
- Noticias (otros idiomas)
- Expertos invitados
- Por especialidad
- de Iberoamérica
- del mundo
- Entrevistas
- Casos clínicos
-
Crónicas de Autores
- Authors’ Reports
-
Instrucciones para autores
-
Expertos Preguntan
- Novedades
- ViASIIC
- Medicina del Dolor
-
Por especialidad
-
Iberomédica
-
Informes comentados
- Textos Completos Autorizados
- Preocupaciones Profesionales
- Red Científica Iberoamericana
- Por materia
- Por fecha
-
Conceptos Categóricos

Casos Clínicos
LA TUBERCULOSIS ES UN DIAGNOSTICO DIFERENCIAL DEL SINDROME SAPHO
Se presenta un caso clínico de tuberculosis pulmonar y extrapulmonar cuya presentación clínica fue similar a la del síndrome SAPHO. Se destaca la necesidad de incluir a la tuberculosis como un diagnóstico diferencial de esta afección, en especial en los pacientes procedentes de áreas endémicas.
Coautores
L Unger* S Wollschläger* M Prinz* T Kittner*
Academic Teaching Hospital Dresden-Friedrichstadt, Dresden, Alemania*
L Unger* S Wollschläger* M Prinz* T Kittner*
Academic Teaching Hospital Dresden-Friedrichstadt, Dresden, Alemania*
Clasificación en siicsalud
Artículos originales > Expertos del Mundo >
página /dato/casiic.php/119148
Especialidades



Artículos originales > Expertos del Mundo >
página /dato/casiic.php/119148
Especialidades
Primera edición en siicsalud
5 de agosto, 2011
5 de agosto, 2011
LA TUBERCULOSIS ES UN DIAGNOSTICO DIFERENCIAL DEL SINDROME SAPHO
(especial para SIIC © Derechos reservados)
(especial para SIIC © Derechos reservados)
Introducción
La sigla SAPHO corresponde a un síndrome definido por sinovitis, acné, pustulosis, hiperostosis y osteítis.1 En los 2 tercios de los pacientes, el compromiso osteoarticular precede a las manifestaciones cutáneas. El dolor en la región anterior del tórax es el signo clínico más frecuente (73%), sucedido de artritis periférica (32%) y dolor sacroilíaco (27%).2 Los parámetros cutáneos típicos incluyen el acné papulopustuloso, la psoriasis pustulosa o las pústulas palmoplantares. Los síntomas extracutáneos y extraosteroarticulares, como el tromboembolismo, pueden complicar tanto el pronóstico como la evolución.3 Se observa predominio del sexo femenino y existe asociación con la enfermedad de Crohn en menos del 10% de los pacientes. Son menos frecuentes la enfermedad de Behçet o las dermatosis neutrofílicas, como el síndrome de Sweet y el pioderma gangrenoso.4 Se observan autoanticuerpos en alrededor del 20% de los pacientes, pero el perfil es inespecífico5 (Grosjean y col, 2010), mientras que el HLA B27 está presente en menos del 5% de los casos.4 No se ha dilucidado el sustrato genético de este síndrome.6 La patogénesis es incierta, aunque se ha sugerido una reacción inflamatoria anormal a patógenos de baja virulencia, como Propionibacterium acnes. En casos infrecuentes, la infección por Treponema pallidum se ha asociado con el síndrome SAPHO.7 Ante el contacto con P. acnes, los niveles plasmáticos de ciertas citoquinas, como las interleuquinas (IL) 8 y 18, se incrementaron, pero se observó una menor producción de factor de necrosis tumoral alfa (TNF-alfa) en los leucocitos mononucleares de sangre periférica.8 Los estudios por imágenes desempeñan un papel relevante en el diagnóstico. La técnica más sensible es la resonancia magnética (RM), sucedida por la tomografía computarizada (TC) y la radiografía convencional. Los hallazgos típicos incluyen la tumefacción de tejidos blandos, la osteoesclerosis, las erosiones de la cortical ósea, el estrechamiento del espacio articular, la esclerosis subcondral, la neoformación ósea en el periostio, la reacción sinovial y el derrame intraarticular. El centellograma óseo demuestra un incremento de la captación en la articulación esternoclavicular.9 El tratamiento puede ser difícil. Las terapias convencionales incluyen los antibióticos, los antiinflamatorios no esteroides (AINE), los corticoides sistémicos, la sulfasalazina, el metotrexato, o la combinación de estos medicamentos.10 Recientemente, se han utilizado en algunos pacientes los inhibidores del TNF-alfa, como el infliximab, el adalimumab o el etanercept.11
Caso clínico
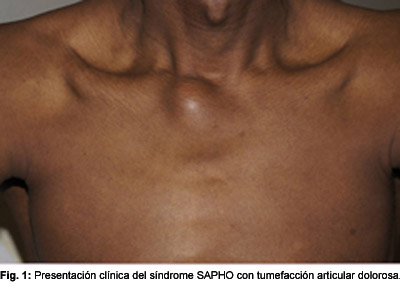
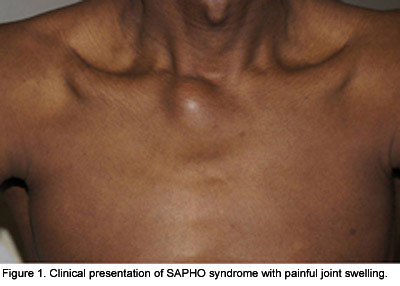
Un estudiante sudanés de 34 años consultó por dolor torácico y acentuada tumefacción de la articulación esternocostoclavicular derecha (Figura 1). Había padecido pérdida de peso durante los meses previos. Seis meses antes había experimentado fiebre de causa inexplicada, sin tos asociada, que había mejorado sin necesidad de medicación. Señaló una internación previa por taquicardia. Se observó derrame pleural y pericárdico, sin signos de tuberculosis a pesar de las evaluaciones pulmonares repetidas y detalladas. En el laboratorio se describió anemia, con valores de hemoglobina de 7.8 mmol/l (valor normal [VN]: 8.6 a 12.1 mmol/l), mayor porcentaje de eritrocitos hipocrómicos (10.3%; VN: menos de 2.5%), trombocitosis (623 000 plaquetas/µl; VN: 120 000 a 340 000 células/µl) y leve linfopenia (18%; VN: 20% a 45%). También se encontraron parámetros de inflamación, como un incremento de los niveles de beta-2-microglobulina (3.3 mg/l; VN: 0.8 a 2.4 mg/l), proteína C-reactiva (73.3 mg/l; VN: menor de 5 mg/l) y eritrosedimentación (79 mm/h; VN: menor de 15 mm/h). Se describió un descenso de las inmunoglobulinas (46.7%; VN: 60.3% a 71.4%) con aumento de las gammaglobulinas (27.9%; VN: 8.7% a 16%). Las determinaciones de anticuerpos para citrulina, anticuerpos antinucleares, p-ANCA, antígeno de superficie para hepatitis B, anticuerpos anticore para hepatitis B y los anticuerpos contra el virus de la hepatitis C, el virus de la inmunodeficiencia humana (VIH) tipos 1 y 2, equinococosis y leishmaniasis fueron en su totalidad negativos. La inmunofijación también fue negativa. El enzimoinmunoensayo (ELISA) para tuberculosis, en cambio, fue positivo.
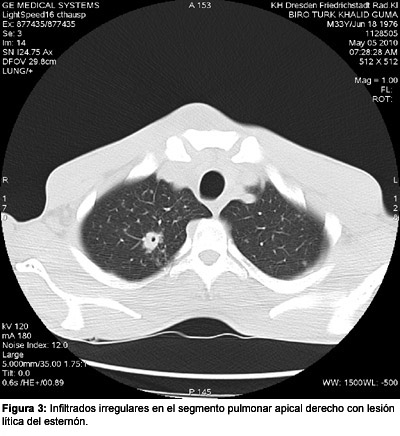
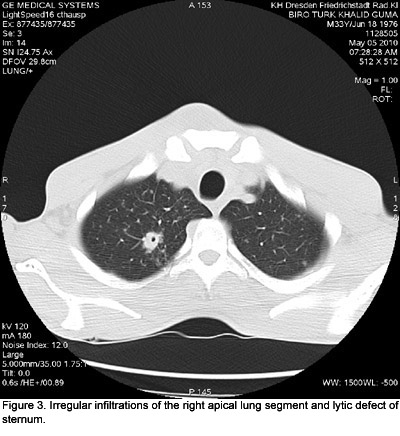
En la RM, se reconoció a nivel preesternal un derrame de 4.5 x 1.5 cm (Figuras 2 y 3). En el lóbulo pulmonar superior derecho se observó una lesión de 1.6 cm de diámetro (Figura 3). En las imágenes por RM de la cabeza y el cuello se reveló un derrame líquido de 4 x 2 x 5 cm, en relación ventral y ventrolateral con las tres primeras vértebras cervicales, compatibles con un absceso (Figura 4). Se detectaron otras 2 lesiones a nivel supraclavicular, sugestivas de una adenopatía o de un absceso (diámetros de 1 y 1.8 cm). No se reconocieron alteraciones en la ecografía abdominal.

La presunción inicial consistió en el síndrome SAPHO, debido a los hallazgos clínicos como la tumefacción articular esternoclavicular y el dolor. Se indicaron 800 mg de ibuprofeno por vía oral. La prueba ELISA para tuberculosis se solicitó para la pesquisa de la enfermedad antes de iniciar un tratamiento con antagonistas del TNF-alfa. El paciente se derivó al servicio de Medicina Interna. Se llevó a cabo la punción de los abscesos de la región esternoclavicular y el hombro izquierdo. Se observaron cocos ácido-alcohol resistentes, con reacción en cadena de la polimerasa (PCR) y cultivo positivos para Mycobacterium tuberculosis. El cultivo de esputo y la PCR del lavado broncoalveolar también fueron positivos para M. tuberculosis.

El diagnóstico final fue reactivación de tuberculosis con compromiso pulmonar y extrapulmonar. Se inició terapia combinada con 250 mg diarios de isoniazida, 1 250 mg diarios de etambutol, 1 500 mg diarios de pirazinamida y 600 mg diarios de rifampicina. Se indicaron también 20 mg/día de vitamina B6. Algunos parámetros de laboratorio y de los estudios por imágenes pulmonares y óseas revelaron optimización durante los meses posteriores. El paciente aumentó de peso y mejoró clínicamente. El tratamiento continuó, si bien los abscesos respondieron en forma muy lenta.
Discusión
Se describe un paciente que se presentó clínicamente como un síndrome SAPHO, aunque se realizó el diagnóstico final de tuberculosis. En la bibliografía se menciona a la tuberculosis de la articulación esternoclavicular como una manifestación extremadamente infrecuente.12-14 Se han recomendado esquemas con 3 o 4 drogas antituberculosas en diversas regiones del mundo, pero el tratamiento conservador sólo es exitoso en las formas precoces.
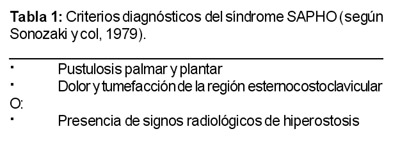
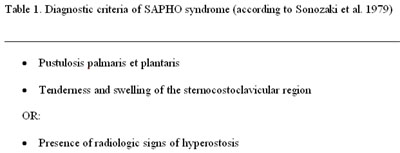
Los hallazgos en las imágenes incluyen destrucción y cambios de la densidad de la señal de huesos y articulaciones, destrucción del cartílago, cambios en los tejidos blandos como la granulación tisular o abscesos y desplazamiento de estructuras adyacentes por celulitis o miositis.15 En relación con los criterios diagnósticos del síndrome SAPHO (Tabla 1), el paciente cumplía sólo con uno de los 3 criterios, correspondiente a la tumefacción de la región esternocostoclavicular.16
La coexistencia del síndrome SAPHO y la tuberculosis ha sido informada recientemente en Japón.17 La identificación de tuberculosis activa simulando un síndrome SAPHO se ha vuelto aún más importante desde que se utilizan los antagonistas del TNF-alfa para el tratamiento del síndrome SAPHO.11 La reactivación de la tuberculosis es un efecto adverso grave de los inhibidores del TNF-alfa.18 Sudán, la nación de origen del paciente de referencia, tiene una alta prevalencia de tuberculosis que ha empeorado durante los conflictos militares de ese país.19 La combinación de absceso tuberculoso, giba y paresia había sido descrita por Percival Pott (1714-1788), quien vivió y ejerció su profesión en Londres (Reino Unido). La asociación se menciona en la bibliografía médica como tríada o enfermedad de Pott. Sin el diagnóstico y el consecuente tratamiento, el paciente hubiera evolucionado con dicha tríada.
El caso clínico expuesto incrementa la presunción de síndrome SAPHO secundario a tuberculosis, en particular en los pacientes que proceden de áreas endémicas, aun si las primeras pruebas diagnósticas para tuberculosis resultan negativas.
Referencias
Chamot AM, Benhamou CL, Kahn MF, et al. Acne-pustulosis-hyperostosis-osteitis syndrome. Results of a national survey. 85 cases. Rev Rhum Mal Osteoartic 54:187-196, 1987. Sallés M, Olivé A, Perez-Andres R, et al. The SAPHO syndrome: a clinical and imaging study. Clin Rheumatol 2010; in press.
Coloe J, Diamantis S, Henderson F, Morrell DS. Synovitis-acne-pustulosis-hyperostosis-osteitis (SAPHO) syndrome complicated by seven pulmonary emboli in a 15-year old patient. J Am Acad Dermatol 62: 333-336, 2010.
Clina M, Govoni M, Orzincolo C, Trotta F. Clinical and radiologic evaluation of sinoviti, acne, pustulosis, hyperostosis, and osteitis syndrome: a single center study of a cohort of 71 subjects. Arthritis Rheum 61: 813-821, 2009.
Grosjean C, Hurtado-Nedelec M, Nicaise-Roland P, et al. Prevalence of autoantibodies in SAPHO syndrome: a single-center study of 90 patients. J Rheumatol 37: 639-643, 2010.
Hurtado-Nemelec M, Chollet-Martin S, Chapeton D, et al. Genetic susceptibility factors in a cohort of 38 patients with SAPHO syndrome: a study of PSTPIP2, NOD2, and LPIN2 genes. J Rheumatol 37: 401-409, 2010.
Arnson Y, Rubinow A, Amital H. Secondary syphilis presenting as SAPHO syndrome features. Clin Exp Rheumatol 26: 1119-1121, 2008.
Hurtado-Nemelec M, Chollet-Martin S, Nicaise-Roland P, et al. Characterization of the immune response in the synovitis, acne, pustulosis, hyperostosis, osteitis (SAPHO) syndrome. Rheumatology (Oxford) 47: 1160-1167, 2008.
Guglielmi G, Cascavilla A, Scalzo G, et al. Imaging of sternocostoclavicular joint in spondyloarthropathies and other rheumatic conditions. Clin Exp Rheumatol 27: 402-408, 2009.
Huber CE, Judex AG, Freyschmidt J, et al. Sequential combination therapy leading to sustained remission in a patient with SAPHO syndrome. Open Rheumatol J 3: 18-21, 2009. Ben Abdelghani K, Dran DG, Gottenberg JE, et al. Tumor necrosis factor-alpha blockers in SAPHO syndrome. J Rheumatol 37: 1699-1704, 2010.
Khan SA, Zahid M, Asif N, Hassan AS. Tuberculosis of the sternoclavicular joint. Indian J Chest Dis Allied Sci 44: 271-273, 2002.
Dhillon MS, Gupta RK, Bahadur R, Nagi ON. Tuberculosis of the sternoclavicular joints. Acta Orthop Scand 72:514-517, 2001. Bezza A, Niamane R, Benbouazza K, et al. Tuberculosis of the sternoclavicular joint. Report of two cases. Rev Rhum Engl Ed 65: 791-794, 1998.
Shah J, Patkar D, Parikh B, et al. Tuberculosis of the sternum and clavicle: imaging findings in 15 patients. Skeletal Radiol 29: 447-453, 2000.
Sonozaki H, Azuma A, Okai K, et al. Clinical features of 22 cases with "inter-sterno-costo-clavicular ossification". A new rheumatic syndrome. Arch Orthop Trauma Surg 95:13-22, 1979.
Nakamura J, Yamada K, Mitsugi N, Saito T. A case of SAPHO syndrome with destructive spondylodiscitis suspicious of tuberculous spondylitis. Mod Rheumatol 20:93-97, 2010.
Wallis RS. Infectious complications of tumor necrosis factor blockade. Curr Opin Infect Dis 22: 403-409, 2009.
Bøhler M, Mustafaa SA, Mørkve O. Tuberculosis treatment outcome and health services: a comparison of displaced and settled population groups in Khartoum, Sudan. Int J Tuberc Lung Dis 9: 32-36, 2005.
La sigla SAPHO corresponde a un síndrome definido por sinovitis, acné, pustulosis, hiperostosis y osteítis.1 En los 2 tercios de los pacientes, el compromiso osteoarticular precede a las manifestaciones cutáneas. El dolor en la región anterior del tórax es el signo clínico más frecuente (73%), sucedido de artritis periférica (32%) y dolor sacroilíaco (27%).2 Los parámetros cutáneos típicos incluyen el acné papulopustuloso, la psoriasis pustulosa o las pústulas palmoplantares. Los síntomas extracutáneos y extraosteroarticulares, como el tromboembolismo, pueden complicar tanto el pronóstico como la evolución.3 Se observa predominio del sexo femenino y existe asociación con la enfermedad de Crohn en menos del 10% de los pacientes. Son menos frecuentes la enfermedad de Behçet o las dermatosis neutrofílicas, como el síndrome de Sweet y el pioderma gangrenoso.4 Se observan autoanticuerpos en alrededor del 20% de los pacientes, pero el perfil es inespecífico5 (Grosjean y col, 2010), mientras que el HLA B27 está presente en menos del 5% de los casos.4 No se ha dilucidado el sustrato genético de este síndrome.6 La patogénesis es incierta, aunque se ha sugerido una reacción inflamatoria anormal a patógenos de baja virulencia, como Propionibacterium acnes. En casos infrecuentes, la infección por Treponema pallidum se ha asociado con el síndrome SAPHO.7 Ante el contacto con P. acnes, los niveles plasmáticos de ciertas citoquinas, como las interleuquinas (IL) 8 y 18, se incrementaron, pero se observó una menor producción de factor de necrosis tumoral alfa (TNF-alfa) en los leucocitos mononucleares de sangre periférica.8 Los estudios por imágenes desempeñan un papel relevante en el diagnóstico. La técnica más sensible es la resonancia magnética (RM), sucedida por la tomografía computarizada (TC) y la radiografía convencional. Los hallazgos típicos incluyen la tumefacción de tejidos blandos, la osteoesclerosis, las erosiones de la cortical ósea, el estrechamiento del espacio articular, la esclerosis subcondral, la neoformación ósea en el periostio, la reacción sinovial y el derrame intraarticular. El centellograma óseo demuestra un incremento de la captación en la articulación esternoclavicular.9 El tratamiento puede ser difícil. Las terapias convencionales incluyen los antibióticos, los antiinflamatorios no esteroides (AINE), los corticoides sistémicos, la sulfasalazina, el metotrexato, o la combinación de estos medicamentos.10 Recientemente, se han utilizado en algunos pacientes los inhibidores del TNF-alfa, como el infliximab, el adalimumab o el etanercept.11
Caso clínico
Un estudiante sudanés de 34 años consultó por dolor torácico y acentuada tumefacción de la articulación esternocostoclavicular derecha (Figura 1). Había padecido pérdida de peso durante los meses previos. Seis meses antes había experimentado fiebre de causa inexplicada, sin tos asociada, que había mejorado sin necesidad de medicación. Señaló una internación previa por taquicardia. Se observó derrame pleural y pericárdico, sin signos de tuberculosis a pesar de las evaluaciones pulmonares repetidas y detalladas. En el laboratorio se describió anemia, con valores de hemoglobina de 7.8 mmol/l (valor normal [VN]: 8.6 a 12.1 mmol/l), mayor porcentaje de eritrocitos hipocrómicos (10.3%; VN: menos de 2.5%), trombocitosis (623 000 plaquetas/µl; VN: 120 000 a 340 000 células/µl) y leve linfopenia (18%; VN: 20% a 45%). También se encontraron parámetros de inflamación, como un incremento de los niveles de beta-2-microglobulina (3.3 mg/l; VN: 0.8 a 2.4 mg/l), proteína C-reactiva (73.3 mg/l; VN: menor de 5 mg/l) y eritrosedimentación (79 mm/h; VN: menor de 15 mm/h). Se describió un descenso de las inmunoglobulinas (46.7%; VN: 60.3% a 71.4%) con aumento de las gammaglobulinas (27.9%; VN: 8.7% a 16%). Las determinaciones de anticuerpos para citrulina, anticuerpos antinucleares, p-ANCA, antígeno de superficie para hepatitis B, anticuerpos anticore para hepatitis B y los anticuerpos contra el virus de la hepatitis C, el virus de la inmunodeficiencia humana (VIH) tipos 1 y 2, equinococosis y leishmaniasis fueron en su totalidad negativos. La inmunofijación también fue negativa. El enzimoinmunoensayo (ELISA) para tuberculosis, en cambio, fue positivo.
En la RM, se reconoció a nivel preesternal un derrame de 4.5 x 1.5 cm (Figuras 2 y 3). En el lóbulo pulmonar superior derecho se observó una lesión de 1.6 cm de diámetro (Figura 3). En las imágenes por RM de la cabeza y el cuello se reveló un derrame líquido de 4 x 2 x 5 cm, en relación ventral y ventrolateral con las tres primeras vértebras cervicales, compatibles con un absceso (Figura 4). Se detectaron otras 2 lesiones a nivel supraclavicular, sugestivas de una adenopatía o de un absceso (diámetros de 1 y 1.8 cm). No se reconocieron alteraciones en la ecografía abdominal.
La presunción inicial consistió en el síndrome SAPHO, debido a los hallazgos clínicos como la tumefacción articular esternoclavicular y el dolor. Se indicaron 800 mg de ibuprofeno por vía oral. La prueba ELISA para tuberculosis se solicitó para la pesquisa de la enfermedad antes de iniciar un tratamiento con antagonistas del TNF-alfa. El paciente se derivó al servicio de Medicina Interna. Se llevó a cabo la punción de los abscesos de la región esternoclavicular y el hombro izquierdo. Se observaron cocos ácido-alcohol resistentes, con reacción en cadena de la polimerasa (PCR) y cultivo positivos para Mycobacterium tuberculosis. El cultivo de esputo y la PCR del lavado broncoalveolar también fueron positivos para M. tuberculosis.
El diagnóstico final fue reactivación de tuberculosis con compromiso pulmonar y extrapulmonar. Se inició terapia combinada con 250 mg diarios de isoniazida, 1 250 mg diarios de etambutol, 1 500 mg diarios de pirazinamida y 600 mg diarios de rifampicina. Se indicaron también 20 mg/día de vitamina B6. Algunos parámetros de laboratorio y de los estudios por imágenes pulmonares y óseas revelaron optimización durante los meses posteriores. El paciente aumentó de peso y mejoró clínicamente. El tratamiento continuó, si bien los abscesos respondieron en forma muy lenta.
Discusión
Se describe un paciente que se presentó clínicamente como un síndrome SAPHO, aunque se realizó el diagnóstico final de tuberculosis. En la bibliografía se menciona a la tuberculosis de la articulación esternoclavicular como una manifestación extremadamente infrecuente.12-14 Se han recomendado esquemas con 3 o 4 drogas antituberculosas en diversas regiones del mundo, pero el tratamiento conservador sólo es exitoso en las formas precoces.
Los hallazgos en las imágenes incluyen destrucción y cambios de la densidad de la señal de huesos y articulaciones, destrucción del cartílago, cambios en los tejidos blandos como la granulación tisular o abscesos y desplazamiento de estructuras adyacentes por celulitis o miositis.15 En relación con los criterios diagnósticos del síndrome SAPHO (Tabla 1), el paciente cumplía sólo con uno de los 3 criterios, correspondiente a la tumefacción de la región esternocostoclavicular.16
La coexistencia del síndrome SAPHO y la tuberculosis ha sido informada recientemente en Japón.17 La identificación de tuberculosis activa simulando un síndrome SAPHO se ha vuelto aún más importante desde que se utilizan los antagonistas del TNF-alfa para el tratamiento del síndrome SAPHO.11 La reactivación de la tuberculosis es un efecto adverso grave de los inhibidores del TNF-alfa.18 Sudán, la nación de origen del paciente de referencia, tiene una alta prevalencia de tuberculosis que ha empeorado durante los conflictos militares de ese país.19 La combinación de absceso tuberculoso, giba y paresia había sido descrita por Percival Pott (1714-1788), quien vivió y ejerció su profesión en Londres (Reino Unido). La asociación se menciona en la bibliografía médica como tríada o enfermedad de Pott. Sin el diagnóstico y el consecuente tratamiento, el paciente hubiera evolucionado con dicha tríada.
El caso clínico expuesto incrementa la presunción de síndrome SAPHO secundario a tuberculosis, en particular en los pacientes que proceden de áreas endémicas, aun si las primeras pruebas diagnósticas para tuberculosis resultan negativas.
Referencias
Chamot AM, Benhamou CL, Kahn MF, et al. Acne-pustulosis-hyperostosis-osteitis syndrome. Results of a national survey. 85 cases. Rev Rhum Mal Osteoartic 54:187-196, 1987. Sallés M, Olivé A, Perez-Andres R, et al. The SAPHO syndrome: a clinical and imaging study. Clin Rheumatol 2010; in press.
Coloe J, Diamantis S, Henderson F, Morrell DS. Synovitis-acne-pustulosis-hyperostosis-osteitis (SAPHO) syndrome complicated by seven pulmonary emboli in a 15-year old patient. J Am Acad Dermatol 62: 333-336, 2010.
Clina M, Govoni M, Orzincolo C, Trotta F. Clinical and radiologic evaluation of sinoviti, acne, pustulosis, hyperostosis, and osteitis syndrome: a single center study of a cohort of 71 subjects. Arthritis Rheum 61: 813-821, 2009.
Grosjean C, Hurtado-Nedelec M, Nicaise-Roland P, et al. Prevalence of autoantibodies in SAPHO syndrome: a single-center study of 90 patients. J Rheumatol 37: 639-643, 2010.
Hurtado-Nemelec M, Chollet-Martin S, Chapeton D, et al. Genetic susceptibility factors in a cohort of 38 patients with SAPHO syndrome: a study of PSTPIP2, NOD2, and LPIN2 genes. J Rheumatol 37: 401-409, 2010.
Arnson Y, Rubinow A, Amital H. Secondary syphilis presenting as SAPHO syndrome features. Clin Exp Rheumatol 26: 1119-1121, 2008.
Hurtado-Nemelec M, Chollet-Martin S, Nicaise-Roland P, et al. Characterization of the immune response in the synovitis, acne, pustulosis, hyperostosis, osteitis (SAPHO) syndrome. Rheumatology (Oxford) 47: 1160-1167, 2008.
Guglielmi G, Cascavilla A, Scalzo G, et al. Imaging of sternocostoclavicular joint in spondyloarthropathies and other rheumatic conditions. Clin Exp Rheumatol 27: 402-408, 2009.
Huber CE, Judex AG, Freyschmidt J, et al. Sequential combination therapy leading to sustained remission in a patient with SAPHO syndrome. Open Rheumatol J 3: 18-21, 2009. Ben Abdelghani K, Dran DG, Gottenberg JE, et al. Tumor necrosis factor-alpha blockers in SAPHO syndrome. J Rheumatol 37: 1699-1704, 2010.
Khan SA, Zahid M, Asif N, Hassan AS. Tuberculosis of the sternoclavicular joint. Indian J Chest Dis Allied Sci 44: 271-273, 2002.
Dhillon MS, Gupta RK, Bahadur R, Nagi ON. Tuberculosis of the sternoclavicular joints. Acta Orthop Scand 72:514-517, 2001. Bezza A, Niamane R, Benbouazza K, et al. Tuberculosis of the sternoclavicular joint. Report of two cases. Rev Rhum Engl Ed 65: 791-794, 1998.
Shah J, Patkar D, Parikh B, et al. Tuberculosis of the sternum and clavicle: imaging findings in 15 patients. Skeletal Radiol 29: 447-453, 2000.
Sonozaki H, Azuma A, Okai K, et al. Clinical features of 22 cases with "inter-sterno-costo-clavicular ossification". A new rheumatic syndrome. Arch Orthop Trauma Surg 95:13-22, 1979.
Nakamura J, Yamada K, Mitsugi N, Saito T. A case of SAPHO syndrome with destructive spondylodiscitis suspicious of tuberculous spondylitis. Mod Rheumatol 20:93-97, 2010.
Wallis RS. Infectious complications of tumor necrosis factor blockade. Curr Opin Infect Dis 22: 403-409, 2009.
Bøhler M, Mustafaa SA, Mørkve O. Tuberculosis treatment outcome and health services: a comparison of displaced and settled population groups in Khartoum, Sudan. Int J Tuberc Lung Dis 9: 32-36, 2005.
Introduction
The acronym SAPHO syndrome refers to synovitis, acne, pustulosis, hyperostosis, and osteitis.1 In two-third of patients osteoarticular involvement is present before cutaneous manifestation. Anterior chest pain is the most common clinical sign (73%) followed by peripheral arthritis (32%) and sacroiliacal pain (27%).2
Typical cutaneous features include papulopustular acne, pustular psoriasis or palmoplantar pustulosis. Extracutaneous and extraosteroarticular symptoms such as thromboembolism may complicate both diagnosis and course.3 The female sex is overrepresented. There is an association with Crohn`s disease in less than 10% of patients. Less common are neutrophilic dermatoses like Sweet’s syndrome and pyoderma gangrenosum, or Behçet’s disease.4
Autoantibodies can be observed in about 20% of patients but their profile is nonspecific5 (Grosjean et al. 2010) whereas HLA B27 is present in less than 5%.4
The genetic background of this syndrome has not been elucidated.6 The pathogenesis is unclear although an abnormal inflammatory reaction to low-virulence pathogens like Propionibacterium acnes has been suggested. In rare cases Treponema pallidum infection has been associated with SAPHO syndrome.7 Plasma levels of certain cytokines like interleukin (IL)-8 and -18 were increased but tumor necrosis factor-alpha (TNFa) production was found to be diminished in peripheral mononuclear blood cells by contact to P. acnes.8
For diagnosis imaging plays a critical role. The most sensitive technique is MRI followed by CT and conventional radiography. Typical findings include soft tissue swelling, bone sclerosis, cortical bone erosions, joint space narrowing, subchondral sclerosis, periosteal new bone formation, synovial reaction and intra-articular effusion. Bone scintigraphy shows an increased uptake at the sterno-clavicular joint.9
Treatment is sometimes difficult. Standard therapies include antibiotics, non-steroidal anti-inflammatory drugs (NSAID), systemic corticosteroids, sulfasalzine, methotrexate or a combination of them.10 Recently TNFa inhibitors like infliximab, adalimumab or etanercept have been used successfully in some patients.11
Case report
A 34-year old Sudanese student presented with chest pain and a marked swelling of his right sternocostoclavicular joint (Fig. 1). He experienced some weight loss during the months. Half a year before he had unexplained fever improved but no coughing. He had been hospitalized before due to tachycardia. Pericardial and pleural effusion was found but no evidence for tuberculosis despite repeated intense pulmonary investigations. Laboratory investigations: Anemia of 7.8 mmol/L (normal range 8.6-12.1 mmol/L), increased percentage of hypochromatic erythrocytes with 10.3% (<2.5%), thrombocytopenia of 623 Gpt/L (120-340 Gpt/L), slight lymphopenia of 18 % (20-45%). Inflammatory signs were present such as increased beta-2-microglobulin of 3.3 mg/L (0.8-2.4 mg/L), C-reactive protein of 73.3 mg/L (< 5mg/L), and blood sedimentation rate of 79 mm/h (< 15 mm/h). Immunoglobulins were decreased with 46.7% (60.3-71.4 %), and gammaglobulins increased to 27.9% (8.7-16 %). He was negative for citrullin antibodies, antinuclear antibodies, p-ANCA, hepatitis Bs antigen, hepatitis BC antibodies, hepatitis C antibodies, HIV 1/2 gO antibodies, echinococcus and leishmaniasis antibodies. Immunofixation was negative as well. TB-spot, however, was positive.
MRI: Presternal we observed a liquid accumulation of 4.5 x 1.5 cm (Figs. 2, 3). In the right upper pulmonary lobe a lesion of 1.6 cm in diameter could be seen (Fig. 3).

MRI of head and neck disclosed a liquid accumulation (4x2x5 cm) ventral and ventrolateral of cervical vertebrae 1 to 3, suggesting an abscess (Fig. 4). Another two lesions were observed supraclavicular suggesting an inflamed lymph node or an abscess (diameter 1 cm and 1.8 cm). Abdominal ultrasound: no pathologic findings.

We primarily suggested a SAPHO syndrome because of clinical findings as sternoclavicular joint swelling and pain. He was given 800mg ibuprofen p.o. The TB spot was performed to screen for tuberculosis before anti-TNFa therapy. The patient was referred to the Department of Internal Medicine.
The abscess of both steronoclavicular region and left shoulder were punctured. Microbial analysis showed acid-fast cocci, Mycobacterium tuberculosis positive polymerase-chain reaction (PCR) and culture. Sputum culture was positive for M. tuberculosis. Bronchoalveolar lavage revealed a M. tuberculosis positive PCR.
The final diagnosis was post-primary tuberculosis with both pulmonary and extrapulmonary manifestation. Anti-infective multidrug therapy was initiated with isoniazid 250 mg/d, ethambutol 1,250 mg/d, pyrazinamide 1,500 mg/d, and rifampicin 600 mg/d. In addition, vitamin B6 20 mg/d was administered. Some laboratory parameters and imaging analysis of pulmonary and bony lesions disclosed improvement during the next months. The patient has gained weight and got better clinically. Treatment is going on, since abscesses will respond only with a marked delay. Discussion
We report about a patient presenting as SAPHO syndrome clinically who was eventually diagnosed as tuberculosis. Tuberculosis of the sternoclavicular joint has been described in the literature as an extremely rare manifestation.12-14 Three to four drug tuberculostatic regimes have been recommended in various parts of the world, but conservative treatment is only successful in early cases.
Imaging findings include destruction and signal density changes of bones and joints, destruction of cartilage, soft tissue changes like granulation tissue or abscess, displacement of adjacent structures by cellulitis or myositis.15 Concerning the diagnostic criteria for SAPHO syndrome (Table 1) our patient fulfilled only one of three criteria, namely swelling of the sternocostoclavicular region.16
The occurrence of SAPHO syndrome and tuberculosis has recently been reported from Japan.17 The recognition of active tuberculosis masquerading as SAPHO syndrome has become even more important, since TNFa inhibitors are now used to treat SAPHO syndrome.11 Reactivation of tuberculosis is a major possible adverse effect of TNFa blockade.18 Sudan, the country of our patient’s origin, has a high prevalence of tuberculosis which has become worse during military conflicts in the country.19
The combination of tubercular abscess, gibbus and paresis had been described by Percival Pott (1714-88), who lived and practised in London/ UK. It is know in medical literature as Pott’s triad or Pott’s disease. Without diagnosis and consequent treatment, our patient would have followed the line of Pott’s triad. Our case report should increase awareness of such SAPHO syndrome due to tuberculosis, in particular in patients from endemic tuberculosis areas, even if the primary investigations for tuberculosis where negative.
The acronym SAPHO syndrome refers to synovitis, acne, pustulosis, hyperostosis, and osteitis.1 In two-third of patients osteoarticular involvement is present before cutaneous manifestation. Anterior chest pain is the most common clinical sign (73%) followed by peripheral arthritis (32%) and sacroiliacal pain (27%).2
Typical cutaneous features include papulopustular acne, pustular psoriasis or palmoplantar pustulosis. Extracutaneous and extraosteroarticular symptoms such as thromboembolism may complicate both diagnosis and course.3 The female sex is overrepresented. There is an association with Crohn`s disease in less than 10% of patients. Less common are neutrophilic dermatoses like Sweet’s syndrome and pyoderma gangrenosum, or Behçet’s disease.4
Autoantibodies can be observed in about 20% of patients but their profile is nonspecific5 (Grosjean et al. 2010) whereas HLA B27 is present in less than 5%.4
The genetic background of this syndrome has not been elucidated.6 The pathogenesis is unclear although an abnormal inflammatory reaction to low-virulence pathogens like Propionibacterium acnes has been suggested. In rare cases Treponema pallidum infection has been associated with SAPHO syndrome.7 Plasma levels of certain cytokines like interleukin (IL)-8 and -18 were increased but tumor necrosis factor-alpha (TNFa) production was found to be diminished in peripheral mononuclear blood cells by contact to P. acnes.8
For diagnosis imaging plays a critical role. The most sensitive technique is MRI followed by CT and conventional radiography. Typical findings include soft tissue swelling, bone sclerosis, cortical bone erosions, joint space narrowing, subchondral sclerosis, periosteal new bone formation, synovial reaction and intra-articular effusion. Bone scintigraphy shows an increased uptake at the sterno-clavicular joint.9
Treatment is sometimes difficult. Standard therapies include antibiotics, non-steroidal anti-inflammatory drugs (NSAID), systemic corticosteroids, sulfasalzine, methotrexate or a combination of them.10 Recently TNFa inhibitors like infliximab, adalimumab or etanercept have been used successfully in some patients.11
Case report
A 34-year old Sudanese student presented with chest pain and a marked swelling of his right sternocostoclavicular joint (Fig. 1). He experienced some weight loss during the months. Half a year before he had unexplained fever improved but no coughing. He had been hospitalized before due to tachycardia. Pericardial and pleural effusion was found but no evidence for tuberculosis despite repeated intense pulmonary investigations. Laboratory investigations: Anemia of 7.8 mmol/L (normal range 8.6-12.1 mmol/L), increased percentage of hypochromatic erythrocytes with 10.3% (<2.5%), thrombocytopenia of 623 Gpt/L (120-340 Gpt/L), slight lymphopenia of 18 % (20-45%). Inflammatory signs were present such as increased beta-2-microglobulin of 3.3 mg/L (0.8-2.4 mg/L), C-reactive protein of 73.3 mg/L (< 5mg/L), and blood sedimentation rate of 79 mm/h (< 15 mm/h). Immunoglobulins were decreased with 46.7% (60.3-71.4 %), and gammaglobulins increased to 27.9% (8.7-16 %). He was negative for citrullin antibodies, antinuclear antibodies, p-ANCA, hepatitis Bs antigen, hepatitis BC antibodies, hepatitis C antibodies, HIV 1/2 gO antibodies, echinococcus and leishmaniasis antibodies. Immunofixation was negative as well. TB-spot, however, was positive.
MRI: Presternal we observed a liquid accumulation of 4.5 x 1.5 cm (Figs. 2, 3). In the right upper pulmonary lobe a lesion of 1.6 cm in diameter could be seen (Fig. 3).
MRI of head and neck disclosed a liquid accumulation (4x2x5 cm) ventral and ventrolateral of cervical vertebrae 1 to 3, suggesting an abscess (Fig. 4). Another two lesions were observed supraclavicular suggesting an inflamed lymph node or an abscess (diameter 1 cm and 1.8 cm). Abdominal ultrasound: no pathologic findings.
We primarily suggested a SAPHO syndrome because of clinical findings as sternoclavicular joint swelling and pain. He was given 800mg ibuprofen p.o. The TB spot was performed to screen for tuberculosis before anti-TNFa therapy. The patient was referred to the Department of Internal Medicine.
The abscess of both steronoclavicular region and left shoulder were punctured. Microbial analysis showed acid-fast cocci, Mycobacterium tuberculosis positive polymerase-chain reaction (PCR) and culture. Sputum culture was positive for M. tuberculosis. Bronchoalveolar lavage revealed a M. tuberculosis positive PCR.
The final diagnosis was post-primary tuberculosis with both pulmonary and extrapulmonary manifestation. Anti-infective multidrug therapy was initiated with isoniazid 250 mg/d, ethambutol 1,250 mg/d, pyrazinamide 1,500 mg/d, and rifampicin 600 mg/d. In addition, vitamin B6 20 mg/d was administered. Some laboratory parameters and imaging analysis of pulmonary and bony lesions disclosed improvement during the next months. The patient has gained weight and got better clinically. Treatment is going on, since abscesses will respond only with a marked delay. Discussion
We report about a patient presenting as SAPHO syndrome clinically who was eventually diagnosed as tuberculosis. Tuberculosis of the sternoclavicular joint has been described in the literature as an extremely rare manifestation.12-14 Three to four drug tuberculostatic regimes have been recommended in various parts of the world, but conservative treatment is only successful in early cases.
Imaging findings include destruction and signal density changes of bones and joints, destruction of cartilage, soft tissue changes like granulation tissue or abscess, displacement of adjacent structures by cellulitis or myositis.15 Concerning the diagnostic criteria for SAPHO syndrome (Table 1) our patient fulfilled only one of three criteria, namely swelling of the sternocostoclavicular region.16
The occurrence of SAPHO syndrome and tuberculosis has recently been reported from Japan.17 The recognition of active tuberculosis masquerading as SAPHO syndrome has become even more important, since TNFa inhibitors are now used to treat SAPHO syndrome.11 Reactivation of tuberculosis is a major possible adverse effect of TNFa blockade.18 Sudan, the country of our patient’s origin, has a high prevalence of tuberculosis which has become worse during military conflicts in the country.19
The combination of tubercular abscess, gibbus and paresis had been described by Percival Pott (1714-88), who lived and practised in London/ UK. It is know in medical literature as Pott’s triad or Pott’s disease. Without diagnosis and consequent treatment, our patient would have followed the line of Pott’s triad. Our case report should increase awareness of such SAPHO syndrome due to tuberculosis, in particular in patients from endemic tuberculosis areas, even if the primary investigations for tuberculosis where negative.
Uwe Wollina, Academic Teaching Hospital Dresden-Friedrichstadt Department of Dermatology and Allergology, 01067, Dresden, Alemania,
e-mail: wollina-uw@khdf.de
1. Chamot AM, Benhamou CL, Kahn MF, et al. Acne-pustulosis-hyperostosis-osteitis syndrome. Results of a national survey. 85 cases. Rev Rhum Mal Osteoartic 1987; 54: 187-96.
2. Sallés M, Olivé A, Perez-Andres R, et al. The SAPHO syndrome: a clinical and imaging study. Clin Rheumatol 2010; in press.
3. Coloe J, Diamantis S, Henderson F, Morrell DS. Synovitis-acne-pustulosis-hyperostosis-osteitis (SAPHO) syndrome complicated by seven pulmonary emboli in a 15-year old patient. J Am Acad Dermatol 2010; 62: 333-6.
4. Clina M, Govoni M, Orzincolo C, Trotta F. Clinical and radiologic evaluation of sinoviti, acne, pustulosis, hyperostosis, and osteitis syndrome: a single center study of a cohort of 71 subjects. Arthritis Rheum 2009; 61: 813-21.
5. Grosjean C, Hurtado-Nedelec M, Nicaise-Roland P, et al. Prevalence of autoantibodies in SAPHO syndrome: a single-center study of 90 patients. J Rheumatol 2010; 37: 639-43.
6. Hurtado-Nemelec M, Chollet-Martin S, Chapeton D, et al. Genetic susceptibility factors in a cohort of 38 patients with SAPHO syndrome: a study of PSTPIP2, NOD2, and LPIN2 genes. J Rheumatol 2010; 37: 401-9.
7. Arnson Y, Rubinow A, Amital H. Secondary syphilis presenting as SAPHO syndrome features. Clin Exp Rheumatol 2008; 26: 1119-21.
8. Hurtado-Nemelec M, Chollet-Martin S, Nicaise-Roland P, et al. Characterization of the immune response in the synovitis, acne, pustulosis, hyperostosis, osteitis (SAPHO) syndrome. Rheumatology (Oxford) 2008; 47: 1160-7.
9. Guglielmi G, Cascavilla A, Scalzo G, et al. Imaging of sternocostoclavicular joint in spondyloarthropathies and other rheumatic conditions. Clin Exp Rheumatol 2009; 27: 402-8.
10. Huber CE, Judex AG, Freyschmidt J, et al. Sequential combination therapy leading to sustained remission in a patient with SAPHO syndrome. Open Rheumatol J 2009; 3: 18-21.
11. Ben Abdelghani K, Dran DG, Gottenberg JE, et al. Tumor necrosis factor-alpha blockers in SAPHO syndrome. J Rheumatol 2010; 37: 1699-704.
12. Khan SA, Zahid M, Asif N, Hassan AS. Tuberculosis of the sternoclavicular joint. Indian J Chest Dis Allied Sci 2002; 44: 271-3.
13. Dhillon MS, Gupta RK, Bahadur R, Nagi ON. Tuberculosis of the sternoclavicular joints. Acta Orthop Scand 2001;72:514-7.
14. Bezza A, Niamane R, Benbouazza K, et al. Tuberculosis of the sternoclavicular joint. Report of two cases. Rev Rhum Engl Ed 1998; 65: 791-4.
15. Shah J, Patkar D, Parikh B, et al. Tuberculosis of the sternum and clavicle: imaging findings in 15 patients. Skeletal Radiol 2000; 29: 447-53.
16. Sonozaki H, Azuma A, Okai K, et al. Clinical features of 22 cases with "inter-sterno-costo-clavicular ossification". A new rheumatic syndrome. Arch Orthop Trauma Surg 1979; 95:13-22.
17. Nakamura J, Yamada K, Mitsugi N, Saito T. A case of SAPHO syndrome with destructive spondylodiscitis suspicious of tuberculous spondylitis. Mod Rheumatol 2010; 20:93-7.
18. Wallis RS. Infectious complications of tumor necrosis factor blockade. Curr Opin Infect Dis 2009; 22: 403-9.
19. Bøhler M, Mustafaa SA, Mørkve O. Tuberculosis treatment outcome and health services: a comparison of displaced and settled population groups in Khartoum, Sudan. Int J Tuberc Lung Dis 2005; 9: 32-6.
Artículos publicados por el autor
(selección)
Wollina U Rosacea and rhinophyma in the elderly Clinics Dermatol 29:61-68, 2011
Wollina U, Haroske G Pyoderma gangrenosum Curr Opin Rheumatol 23:50-56, 2011
Hansel G, Schönlebe J, Haroske G, Wollina U Late recurrence (10 years or more) of malignant melanoma in south-east Germany (Saxony). A single-centre analysis of 1,881 patients with a follow-up of 10 years or more J Eur Acad Dermatol Venereol 24:833-836, 2010
Solís D, Maté MJ, Lohr M, Ribeiro J, López-Merino L, André S, Buzament E, Cañada FJ, Kaltner y col. N-Domain of human adhesion/growth-regulatory galectin-9, a monomeric protein with characteristic localization in colon cancer and melanoma: selectivity for ligand conformers/type of cell surface glycoconjugate and detection of ligand-induced structural changes in crystal and in solution Int J Biochem Cell Biol 42:1019-1029, 2010
Verma SB, Wollina U Acne keloidalis nuchae: more than a casual association with metabolic syndrome, truncal obesity and impending/overt diabetes? Am J Clin Dermatol 11:433-436, 2010
Wollina U Pompholyx. A review of clinical features, differential diagnosis and management. Am J Clin Dermatol 11:305-314, 2010
Wollina U Bilateral milia en plaque of the eyelids, long eyelashes and unibrow - case report and review of literature. Dermatol Surg 36:406-408, 2010
Wollina U Ablative erbium:YAG laser treatment of idiopathic chronic inflammatory non-cicatrical balanoposthitis (Zoon's disease) - a series of 20 patients with long-term outcome. J Cosm Laser Ther 12:120-123, 2010
Wollina U Riga-Feede-like disease in a 70-year-old woman - case report and treatment. Indian J Dermatol 55:92-94, 2010
Wollina U, Bayyoud Y Reconstruction of a large scalp defect by sequential use of dermal substitute, self-filling osmotic tissue expander and rotational flap. J Cutan Aesth Surg 3:106-110, 2010
Wollina U, Goldman A, Heinig B Microcannular tumescent liposuction in advanced lipoedema and Dercum's disease. G Ital Dermatol Venereol 145:151-159, 2010
Wollina U, Hansel G, Krönert C, Heinig B Using VAC to facilitate healing of traumatic wounds in patients with chronic lymphoedema. J Wound Care 19:15-17, 2010
Wollina U, Pabst F, Krönert C, Schorcht J, Haroske G, Kittner T High-risk basal cell carcinoma: an update. Expert Rev Dermatol 5:357-368, 2010
Wollina U, Payne CR Aging well - the role of minimally invasive aesthetic dermatological procedures in women over 65. J Cosmet Dermatol 9:50-58, 2010
Wollina U, Unger L, Heinig B, Kittner T Psoriatic arthritis. Dermatol Ther 23:123-136, 2010
Wollina U Rosacea and rhinophyma in the elderly Clinics Dermatol 29:61-68, 2011
Wollina U, Haroske G Pyoderma gangrenosum Curr Opin Rheumatol 23:50-56, 2011
Hansel G, Schönlebe J, Haroske G, Wollina U Late recurrence (10 years or more) of malignant melanoma in south-east Germany (Saxony). A single-centre analysis of 1,881 patients with a follow-up of 10 years or more J Eur Acad Dermatol Venereol 24:833-836, 2010
Solís D, Maté MJ, Lohr M, Ribeiro J, López-Merino L, André S, Buzament E, Cañada FJ, Kaltner y col. N-Domain of human adhesion/growth-regulatory galectin-9, a monomeric protein with characteristic localization in colon cancer and melanoma: selectivity for ligand conformers/type of cell surface glycoconjugate and detection of ligand-induced structural changes in crystal and in solution Int J Biochem Cell Biol 42:1019-1029, 2010
Verma SB, Wollina U Acne keloidalis nuchae: more than a casual association with metabolic syndrome, truncal obesity and impending/overt diabetes? Am J Clin Dermatol 11:433-436, 2010
Wollina U Pompholyx. A review of clinical features, differential diagnosis and management. Am J Clin Dermatol 11:305-314, 2010
Wollina U Bilateral milia en plaque of the eyelids, long eyelashes and unibrow - case report and review of literature. Dermatol Surg 36:406-408, 2010
Wollina U Ablative erbium:YAG laser treatment of idiopathic chronic inflammatory non-cicatrical balanoposthitis (Zoon's disease) - a series of 20 patients with long-term outcome. J Cosm Laser Ther 12:120-123, 2010
Wollina U Riga-Feede-like disease in a 70-year-old woman - case report and treatment. Indian J Dermatol 55:92-94, 2010
Wollina U, Bayyoud Y Reconstruction of a large scalp defect by sequential use of dermal substitute, self-filling osmotic tissue expander and rotational flap. J Cutan Aesth Surg 3:106-110, 2010
Wollina U, Goldman A, Heinig B Microcannular tumescent liposuction in advanced lipoedema and Dercum's disease. G Ital Dermatol Venereol 145:151-159, 2010
Wollina U, Hansel G, Krönert C, Heinig B Using VAC to facilitate healing of traumatic wounds in patients with chronic lymphoedema. J Wound Care 19:15-17, 2010
Wollina U, Pabst F, Krönert C, Schorcht J, Haroske G, Kittner T High-risk basal cell carcinoma: an update. Expert Rev Dermatol 5:357-368, 2010
Wollina U, Payne CR Aging well - the role of minimally invasive aesthetic dermatological procedures in women over 65. J Cosmet Dermatol 9:50-58, 2010
Wollina U, Unger L, Heinig B, Kittner T Psoriatic arthritis. Dermatol Ther 23:123-136, 2010
Está expresamente prohibida la redistribución y la redifusión de todo o parte de los
contenidos de la Sociedad Iberoamericana de Información Científica (SIIC) S.A. sin
previo y expreso consentimiento de SIIC.
ua91218

