


-
 Alergia
Alergia -
 Anestesiología
Anestesiología -
 Bioquímica
Bioquímica
-
 Cardiología
Cardiología
-
 Cirugía
Cirugía
-
 Dermatología
Dermatología
-
 Endocrinología y Metabolismo
Endocrinología y Metabolismo
-
 Enfermería
Enfermería
-
 Gastroenterología
Gastroenterología
-
 Hematología
Hematología
-
 Infectología
Infectología
-
 Inmunología
Inmunología
-
 Medicina Interna
Medicina Interna
-
 Nefrología
Nefrología
-
 Neumonología
Neumonología
-
 Neurología
Neurología
-
 Nutrición
Nutrición
-
 Obstetricia y Ginecología
Obstetricia y Ginecología
-
 Odontología
Odontología
-
 Oncología
Oncología
-
 Otorrinolaringología
Otorrinolaringología
-
 Pediatría
Pediatría
-
 Salud Mental
Salud Mental
-
 Salud Pública
Salud Pública
-
 Urología
Urología
-
 Más Especialidades
Más Especialidades
- Índice
-
Acceso por especialidad
-
Alergia
-
Anestesiología
-
Bioquímica
-
Cardiología
-
Cirugía
-
Dermatología
-
Endocrinología y Metabolismo
-
Enfermería
-
Gastroenterología
-
Hematología
-
Infectología
-
Inmunología
-
Medicina Interna
-
Nefrología
-
Neumonología
-
Neurología
-
Nutrición
-
Obstetricia y Ginecología
-
Odontología
-
Oncología
-
Otorrinolaringología
-
Pediatría
-
Salud Mental
-
Salud Pública
-
Urología
-
Más Especialidades
-
Noticias biomédicas

-
Fuentes informativas
- Editoriales
-
COVID-19
-
INFORMES CIENTÍFICOS
- Preguntas con Respuesta
- América Latina Investiga
- Completos revisados (full text)
-
NOTICIAS/OPINIONES
-
Expertos invitados
- Por especialidad
- de Iberoamérica
- del mundo
- Entrevistas
- Casos clínicos
-
Crónicas de Autores
- Authors’ Reports
-
Instrucciones para autores
-
Expertos Preguntan
-
Novedades
- ViASIIC
- Medicina del Dolor
-
Por especialidad
-
Iberomédica
-
Informes comentados
- Textos Completos Autorizados
- Preocupaciones Profesionales
-
Red Científica Iberoamericana (RedCIbe)
-
Conceptos Categoricos
-
Acceso por especialidad

-
Alergia
-
Anestesiología
-
Bioquímica
-
Cardiología
-
Cirugía
-
Dermatología
-
Endocrinología y Metabolismo
-
Enfermería
-
Gastroenterología
-
Hematología
-
Infectología
-
Inmunología
-
Medicina Interna
-
Nefrología
-
Neumonología
-
Neurología
-
Nutrición
-
Obstetricia y Ginecología
-
Odontología
-
Oncología
-
Otorrinolaringología
-
Pediatría
-
Salud Mental
-
Salud Pública
-
Urología
-
Más Especialidades
-
Noticias biomédicas
-
Fuentes informativas
- Editoriales
- Covid-19
-
Informes Científicos
- Preguntas con Respuesta
- América Latina Investiga
- Completos revisados (full text)
- Noticias/Opiniones
- Noticias (castellano/portugués)
- Noticias (otros idiomas)
- Expertos invitados
- Por especialidad
- de Iberoamérica
- del mundo
- Entrevistas
- Casos clínicos
-
Crónicas de Autores
- Authors’ Reports
-
Instrucciones para autores
-
Expertos Preguntan
- Novedades
- ViASIIC
- Medicina del Dolor
-
Por especialidad
-
Iberomédica
-
Informes comentados
- Textos Completos Autorizados
- Preocupaciones Profesionales
- Red Científica Iberoamericana
- Por materia
- Por fecha
-
Conceptos Categóricos

Casos Clínicos
MASTOCITOSIS SISTEMICA ASOCIADA CON LA LEUCEMIA MIELOIDE AGUDA
El dasatinib parece asociarse con una adecuada respuesta hematológica en quienes coexiste una mastocitosis sistémica y una neoplasia hematológica. Los nuevos inhibidores de la tirosina quinasa representan una alternativa para optimizar el pronóstico de estos enfermos.
Coautores
Kapil Bhalla*
Medical College of Georgia, Augusta, EE.UU.*
Kapil Bhalla*
Medical College of Georgia, Augusta, EE.UU.*
Clasificación en siicsalud
Artículos originales > Expertos del Mundo >
página /dato/casiic.php/115087
Especialidades



Artículos originales > Expertos del Mundo >
página /dato/casiic.php/115087
Especialidades
Primera edición en siicsalud
18 de enero, 2011
18 de enero, 2011
MASTOCITOSIS SISTEMICA ASOCIADA CON LA LEUCEMIA MIELOIDE AGUDA
(especial para SIIC © Derechos reservados)
(especial para SIIC © Derechos reservados)
Introducción
La mastocitosis sistémica (MS), una proliferación clonal de mastocitos, es definida por la Organización Mundial de la Salud (OMS) como la infiltración de estas células en al menos un órgano extracutáneo, en presencia o en ausencia de signos de compromiso cutáneo.1 La MS es una enfermedad muy heterogénea, que incluye formas indolentes con una expectativa de vida normal.1,2 También se describen formas virulentas, como la MS agresiva (MSA), el sarcoma de mastocitos y la leucemia mastocítica.1,2 La MS asociada con una proliferación clonal hematológica de estirpe diferente de la mastocítica (MS-NHNM) constituye un 20% a un 30% de los casos.1,2 La evolución de los pacientes con esta asociación depende de manera fundamental del pronóstico de la neoplasia hematológica concurrente.
Se informó que casi todas las neoplasias hematológicas, con la excepción de la enfermedad de Hodgkin, se asocian con la MS.3,8 Las afecciones más frecuentemente vinculadas con la MS son las de estirpe mieloide, como la leucemia mieloblástica aguda (LMA), la leucemia mielomonocítica crónica y la leucemia mieloide crónica (LMC).3 Recientemente se informó de la coexistencia de dos neoplasias hematológicas en un enfermo con MS.9 Más del 90% de los pacientes con MS presentan una mutación puntual activadora en la proteína KIT. Este receptor de la tirosina quinasa de clase III incluye un dominio extracelular con cinco secuencias repetidas similares a las de las inmunoglobulinas, un único dominio de transmembrana, un dominio de yuxtamembrana y dominio citoplasmático de tirosina quinasa.10 La mutación puntual más frecuente, KITD816V, es el resultado de la sustitución de la valina por asparagina en el codón 816 del exón 17 del gen KIT.11 Debido a la activación independiente del ligando de la tirosina quinasa KIT, el imatinib (un inhibidor de la tirosina quinasa [ITQ]), considerado el tratamiento de elección para la LMC, se utiliza a menudo en la MS.11-13 Sin embargo, puede resultar un terapia ineficaz.11-13 El dasatinib, un ITQ de segunda línea en el tratamiento de la LMC, se utiliza también en pacientes con MS.14,15 Publicamos un caso clínico en el cual el dasatinib y la quimioterapia se asociaron con supervivencia a largo plazo.15 De mayor interés resulta que la mutación KITD816V fue indetectable después del tratamiento (el caso clínico completo está disponible en Leukemia Research). Aquí se describe un resumen del tratamiento y la actualización.
Caso clínico
Un varón de 51 años se presentó a la consulta con astenia, dolor abdominal y pérdida de peso en enero de 2007. Se realizó una biopsia con aspiración de la médula ósea debido a la detección de blastos en sangre periférica. Se reconocieron dos poblaciones celulares diferentes: mieloblastos (positivos para HLA-DR, CD34 y CD13) y mastocitos redondeados o fusiformes (positivos para CD25, CD117, CD64, HLA-DR, CD13, CD33, CD36, mieloperoxidasa y CD11c; negativos para CD34). El cariotipo fue normal en los estudios citogenéticos y moleculares. Mediante la secuenciación bidireccional del exón 17 del gen KIT se demostró una mutación D816V en la muestra diagnóstica de la médula ósea. En una tomografía computarizada de abdomen y pelvis se observó hepatoesplenomegalia, linfadenopatías y lesiones líticas en la pelvis ósea. Se diagnosticó MS-NHNM (MS y LMA). El diagnóstico de SM se fundamentó en la presencia de un criterio mayor (más de 15 agregados de mastocitos en la médula ósea) y cuatro criterios menores de la OMS (morfología fusiforme, positividad para CD25, presencia de la mutación KITD816V, elevación de la triptasa sérica). El paciente alcanzó una remisión hematológica completa con reinducción en términos de la LMA. Los mastocitos permanecían en la médula ósea durante la remisión. El enfermo continuó la terapia de consolidación con altas dosis de citarabina debido a la falta de disponibilidad de TCMH alogénico para su caso. Se adicionó dasatinib (como cortesía de Bristol-Myers Squibb en el marco de su programa de sostenimiento de pacientes) a la terapia de consolidación en una dosis de 70 mg, 2 veces al día.
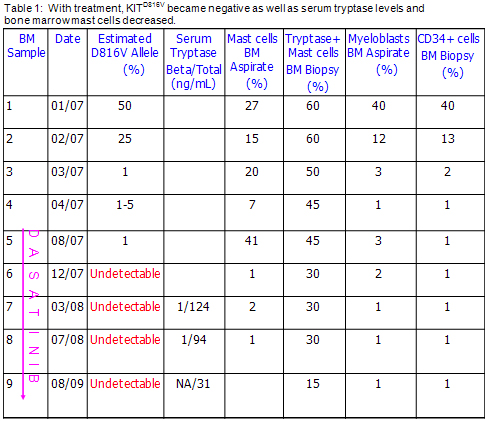
La terapia de mantenimiento con dasatinib se mantiene hasta la actualidad. Debido a la aparición de citopenias leves o moderadas, se redujo la dosis a 50 mg diarios. Desde el punto de vista morfológico, el paciente permaneció en respuesta hematológica completa en relación con la LMA, y en respuesta parcial para la MS. Las lesiones óseas líticas mejoraron levemente según se observó en tomografías computarizadas repetidas. La mutación KITD816V se hizo indetectable (Tabla 1). En la última biopsia de médula ósea, efectuada un año después de la publicación, se confirmaron los mismos resultados (Tabla 1). En una reciente biopsia hepática de este paciente, realizada por una elevación de las enzimas hepáticas, se describió infiltración por mastocitos y fibrosis periportal en estadio II/III. Fue posible efectuar un análisis in vitro de las células CD34+ (incluidos los mieloblastos) y CD34- (incluidos los mastocitos). En ambos tipos celulares se confirmó la presencia de la mutación KITD816V al momento del diagnóstico, aunque se negativizó con el tratamiento. Las pruebas para la mutación c-KIT se realizaron en dos laboratorios independientes con resultados coincidentes. Además, la terapia con dasatinib redujo la actividad de STAT5, STAT3, AKT y ERK y se vinculó con una disminución de los niveles de c-KIT en las células CD34-, con inducción de pérdida de la viabilidad de estos elementos celulares.

Discusión
La MSA se asocia con mal pronóstico. Los pacientes requieren terapia de citorreducción.1,2 El interferón alfa y la cladribina son los medicamentos citorreductores que se utilizan con mayor frecuencia,1,2 pero la tasa de respuesta global es de alrededor de 50% a 60%, con menores índices de respuesta completa con estos fármacos.1,2,16 Los ITQ se convirtieron en una alternativa de interés, debido a que no se dispone de una terapia estandarizada de la MSA. El primer ITQ utilizado en la MS fue el imatinib. Este medicamento es eficaz en modelos de MS in vitro o in vivo sin mutaciones o en presencia de ciertas mutaciones como la del receptor del factor de crecimiento derivado de las plaquetas (PDGFR). No obstante, el imatinib no es activo en presencia de la mutación KITD816V.17-34 Esta falta de eficacia se atribuye a cambios en la conformación del sitio de activación yuxtapuesto en la entrada del bolsillo enzimático de la KIT, los cuales interfieren con la unión del imatinib.17-20 En un ensayo de fase II, 20 pacientes recibieron 400 mg diarios de imatinib durante una mediana de nueve meses.24 Sólo en un enfermo (MS con síndrome hipereosinofílico sin la mutación KITD816V) se observó respuesta hematológica completa, mientras que en seis sujetos se describió mejoría sintomática y en 13 pacientes no se obtuvo respuesta. Un grupo italiano efectuó un análisis retrospectivo de 24 enfermos con MS avanzada. El imatinib fue el medicamento más utilizado en estos individuos (29%).25 La tasa de respuesta fue baja (una respuesta hematológica completa y cuatro respuestas parciales). Se destaca que en ninguno de los pacientes que respondieron al tratamiento se diagnosticó la presencia de la mutación KITD816V. En un estudio diferente, Pardanini y col. demostraron respuesta global en cinco casos en un grupo de diez enfermos. Ninguno de los individuos que respondieron al tratamiento expresaba la mutación KITD816V.26 En contraposición con estos ensayos, en un estudio de fase II se verificó la eficacia clínica del imatinib (reducción de al menos dos criterios de valoración del protocolo) en todos los pacientes con la mutación KITD816V.27 Los criterios de valoración habían sido la triptasa sérica, la excreción urinaria de N-metil-histamina, las lesiones cutáneas, la cantidad de mastocitos en los preparados de médula ósea, los síntomas y la presencia de hepatomegalia, esplenomegalia o ambas.27 En este caso, se administraron 400 mg de imatinib una vez al día por 3 a 16 meses en 14 enfermos. Once de estos pacientes tenían la mutación KITD816V.
Muchos resultados disponibles en la bibliografía acerca del uso de dasatinib en sujetos con MS son relativamente desalentadores. En un estudio de fase II, el dasatinib se relacionó con una respuesta global del 30% en 33 pacientes con MS (18 formas indolentes, nueve casos de MSA y seis con enfermedades hematológicas asociadas).14 De los seis sujetos con enfermedades hematológicas, se describió una respuesta mayor al dasatinib en tres casos, pero la mayor parte (4/6) fallecieron, uno de ellos como consecuencia de progresión de la LMA. De los dos individuos con MS-NHNM (uno con mielofibrosis y otro con síndrome hipereosinofílico) en quienes se logró una respuesta hematológica completa, ninguno presentaba la mutación KITD816V. El sujeto con mielofibrosis evolucionó posteriormente con LMA y falleció. En otro estudio, se administró dasatinib a cuatro pacientes con MS sin enfermedades hematológicas asociadas.35 Dos de estos sujetos presentaron una mejoría sintomática inicial, pero luego evolucionaron con LMA y fallecieron. En un estudio diferente, se observó optimización de los síntomas en un individuo con MS-NHNM tratado con dasatinib.36 En otro ensayo, un enfermo con MSA falleció rápidamente a pesar de la terapia con cladribina y dasatinib.37 Nuestro paciente fue el caso con mejor respuesta al tratamiento con dasatinib (en combinación con la quimioterapia) mencionado en la bibliografía.15 La LMA de este enfermo ha permanecido en remisión hematológica completa por más de 42 meses. Desde el punto de vista morfológico, el recuento de mastocitos disminuyó significativamente. Se hace énfasis en que se logró una remisión molecular (la mutación KITD816V se convirtió en indetectable). La remisión molecular se ha preservado con la terapia de mantenimiento con dasatinib en este paciente. Este resultado indica que no todos los mastocitos neoplásicos contienen la mutación KITD816V o, en otros términos, los mastocitos son heterogéneos y, a diferencia de lo señalado en la LMC, la supervivencia de los mastocitos neoplásicos depende de más de una aberración genética.
La midostaurina (PKC412) aparece como el ITQ más promisorio para el tratamiento de la MS. En un estudio de fase II, Gotlib y col. demostraron que la administración de 100 mg de midostaurina 2 veces al día se asoció con una respuesta global del 73% en 15 pacientes con MSA (cinco de ellos con respuesta mayor y otros seis con respuesta parcial).38 El nilotinib fue activo contra los mastocitos con c-KIT natural o aquellos con la mutación yuxtamembrana D560G de este gen, pero no lo fue en aquellos mastocitos que expresaban la tirosina quinasa con la mutación KITD816V.39 En un estudio de fase II se evaluó el uso de 400 mg de nilotinib 2 veces al día en 60 pacientes con MS.40 La mutación KITD816V fue positiva en el 83% de los 36 enfermos en los cuales se estudió su presencia. La respuesta global sólo se confirmó en doce de esos sujetos (20%).
Se considera importante determinar la respuesta a los ITQ en pacientes con MS-NHNM. En algunos informes se señaló que las células hematológicas malignas asociadas presentan la misma mutación en el gen KIT.15,41-45 Este hallazgo permite avalar el concepto de un progenitor neoplásico común para los mastocitos neoplásicos y las células hematológicas malignas. En consecuencia, tanto la MS como la neoplasia hematológica podrían mejorar con el uso de ITQ en los sujetos con MS-NHNM.
En nuestro paciente, la combinación de dasatinib y quimioterapia provocó la eliminación de los mieloblastos y los mastocitos neoplásicos portadores de la mutación KITD816V. Consideramos que el dasatinib mejoró la evolución de este enfermo en el contexto de una afección que se caracteriza por un muy mal pronóstico.
Los autores no manifiestan conflictos de intereses.
La mastocitosis sistémica (MS), una proliferación clonal de mastocitos, es definida por la Organización Mundial de la Salud (OMS) como la infiltración de estas células en al menos un órgano extracutáneo, en presencia o en ausencia de signos de compromiso cutáneo.1 La MS es una enfermedad muy heterogénea, que incluye formas indolentes con una expectativa de vida normal.1,2 También se describen formas virulentas, como la MS agresiva (MSA), el sarcoma de mastocitos y la leucemia mastocítica.1,2 La MS asociada con una proliferación clonal hematológica de estirpe diferente de la mastocítica (MS-NHNM) constituye un 20% a un 30% de los casos.1,2 La evolución de los pacientes con esta asociación depende de manera fundamental del pronóstico de la neoplasia hematológica concurrente.
Se informó que casi todas las neoplasias hematológicas, con la excepción de la enfermedad de Hodgkin, se asocian con la MS.3,8 Las afecciones más frecuentemente vinculadas con la MS son las de estirpe mieloide, como la leucemia mieloblástica aguda (LMA), la leucemia mielomonocítica crónica y la leucemia mieloide crónica (LMC).3 Recientemente se informó de la coexistencia de dos neoplasias hematológicas en un enfermo con MS.9 Más del 90% de los pacientes con MS presentan una mutación puntual activadora en la proteína KIT. Este receptor de la tirosina quinasa de clase III incluye un dominio extracelular con cinco secuencias repetidas similares a las de las inmunoglobulinas, un único dominio de transmembrana, un dominio de yuxtamembrana y dominio citoplasmático de tirosina quinasa.10 La mutación puntual más frecuente, KITD816V, es el resultado de la sustitución de la valina por asparagina en el codón 816 del exón 17 del gen KIT.11 Debido a la activación independiente del ligando de la tirosina quinasa KIT, el imatinib (un inhibidor de la tirosina quinasa [ITQ]), considerado el tratamiento de elección para la LMC, se utiliza a menudo en la MS.11-13 Sin embargo, puede resultar un terapia ineficaz.11-13 El dasatinib, un ITQ de segunda línea en el tratamiento de la LMC, se utiliza también en pacientes con MS.14,15 Publicamos un caso clínico en el cual el dasatinib y la quimioterapia se asociaron con supervivencia a largo plazo.15 De mayor interés resulta que la mutación KITD816V fue indetectable después del tratamiento (el caso clínico completo está disponible en Leukemia Research). Aquí se describe un resumen del tratamiento y la actualización.
Caso clínico
Un varón de 51 años se presentó a la consulta con astenia, dolor abdominal y pérdida de peso en enero de 2007. Se realizó una biopsia con aspiración de la médula ósea debido a la detección de blastos en sangre periférica. Se reconocieron dos poblaciones celulares diferentes: mieloblastos (positivos para HLA-DR, CD34 y CD13) y mastocitos redondeados o fusiformes (positivos para CD25, CD117, CD64, HLA-DR, CD13, CD33, CD36, mieloperoxidasa y CD11c; negativos para CD34). El cariotipo fue normal en los estudios citogenéticos y moleculares. Mediante la secuenciación bidireccional del exón 17 del gen KIT se demostró una mutación D816V en la muestra diagnóstica de la médula ósea. En una tomografía computarizada de abdomen y pelvis se observó hepatoesplenomegalia, linfadenopatías y lesiones líticas en la pelvis ósea. Se diagnosticó MS-NHNM (MS y LMA). El diagnóstico de SM se fundamentó en la presencia de un criterio mayor (más de 15 agregados de mastocitos en la médula ósea) y cuatro criterios menores de la OMS (morfología fusiforme, positividad para CD25, presencia de la mutación KITD816V, elevación de la triptasa sérica). El paciente alcanzó una remisión hematológica completa con reinducción en términos de la LMA. Los mastocitos permanecían en la médula ósea durante la remisión. El enfermo continuó la terapia de consolidación con altas dosis de citarabina debido a la falta de disponibilidad de TCMH alogénico para su caso. Se adicionó dasatinib (como cortesía de Bristol-Myers Squibb en el marco de su programa de sostenimiento de pacientes) a la terapia de consolidación en una dosis de 70 mg, 2 veces al día.
La terapia de mantenimiento con dasatinib se mantiene hasta la actualidad. Debido a la aparición de citopenias leves o moderadas, se redujo la dosis a 50 mg diarios. Desde el punto de vista morfológico, el paciente permaneció en respuesta hematológica completa en relación con la LMA, y en respuesta parcial para la MS. Las lesiones óseas líticas mejoraron levemente según se observó en tomografías computarizadas repetidas. La mutación KITD816V se hizo indetectable (Tabla 1). En la última biopsia de médula ósea, efectuada un año después de la publicación, se confirmaron los mismos resultados (Tabla 1). En una reciente biopsia hepática de este paciente, realizada por una elevación de las enzimas hepáticas, se describió infiltración por mastocitos y fibrosis periportal en estadio II/III. Fue posible efectuar un análisis in vitro de las células CD34+ (incluidos los mieloblastos) y CD34- (incluidos los mastocitos). En ambos tipos celulares se confirmó la presencia de la mutación KITD816V al momento del diagnóstico, aunque se negativizó con el tratamiento. Las pruebas para la mutación c-KIT se realizaron en dos laboratorios independientes con resultados coincidentes. Además, la terapia con dasatinib redujo la actividad de STAT5, STAT3, AKT y ERK y se vinculó con una disminución de los niveles de c-KIT en las células CD34-, con inducción de pérdida de la viabilidad de estos elementos celulares.
Discusión
La MSA se asocia con mal pronóstico. Los pacientes requieren terapia de citorreducción.1,2 El interferón alfa y la cladribina son los medicamentos citorreductores que se utilizan con mayor frecuencia,1,2 pero la tasa de respuesta global es de alrededor de 50% a 60%, con menores índices de respuesta completa con estos fármacos.1,2,16 Los ITQ se convirtieron en una alternativa de interés, debido a que no se dispone de una terapia estandarizada de la MSA. El primer ITQ utilizado en la MS fue el imatinib. Este medicamento es eficaz en modelos de MS in vitro o in vivo sin mutaciones o en presencia de ciertas mutaciones como la del receptor del factor de crecimiento derivado de las plaquetas (PDGFR). No obstante, el imatinib no es activo en presencia de la mutación KITD816V.17-34 Esta falta de eficacia se atribuye a cambios en la conformación del sitio de activación yuxtapuesto en la entrada del bolsillo enzimático de la KIT, los cuales interfieren con la unión del imatinib.17-20 En un ensayo de fase II, 20 pacientes recibieron 400 mg diarios de imatinib durante una mediana de nueve meses.24 Sólo en un enfermo (MS con síndrome hipereosinofílico sin la mutación KITD816V) se observó respuesta hematológica completa, mientras que en seis sujetos se describió mejoría sintomática y en 13 pacientes no se obtuvo respuesta. Un grupo italiano efectuó un análisis retrospectivo de 24 enfermos con MS avanzada. El imatinib fue el medicamento más utilizado en estos individuos (29%).25 La tasa de respuesta fue baja (una respuesta hematológica completa y cuatro respuestas parciales). Se destaca que en ninguno de los pacientes que respondieron al tratamiento se diagnosticó la presencia de la mutación KITD816V. En un estudio diferente, Pardanini y col. demostraron respuesta global en cinco casos en un grupo de diez enfermos. Ninguno de los individuos que respondieron al tratamiento expresaba la mutación KITD816V.26 En contraposición con estos ensayos, en un estudio de fase II se verificó la eficacia clínica del imatinib (reducción de al menos dos criterios de valoración del protocolo) en todos los pacientes con la mutación KITD816V.27 Los criterios de valoración habían sido la triptasa sérica, la excreción urinaria de N-metil-histamina, las lesiones cutáneas, la cantidad de mastocitos en los preparados de médula ósea, los síntomas y la presencia de hepatomegalia, esplenomegalia o ambas.27 En este caso, se administraron 400 mg de imatinib una vez al día por 3 a 16 meses en 14 enfermos. Once de estos pacientes tenían la mutación KITD816V.
Muchos resultados disponibles en la bibliografía acerca del uso de dasatinib en sujetos con MS son relativamente desalentadores. En un estudio de fase II, el dasatinib se relacionó con una respuesta global del 30% en 33 pacientes con MS (18 formas indolentes, nueve casos de MSA y seis con enfermedades hematológicas asociadas).14 De los seis sujetos con enfermedades hematológicas, se describió una respuesta mayor al dasatinib en tres casos, pero la mayor parte (4/6) fallecieron, uno de ellos como consecuencia de progresión de la LMA. De los dos individuos con MS-NHNM (uno con mielofibrosis y otro con síndrome hipereosinofílico) en quienes se logró una respuesta hematológica completa, ninguno presentaba la mutación KITD816V. El sujeto con mielofibrosis evolucionó posteriormente con LMA y falleció. En otro estudio, se administró dasatinib a cuatro pacientes con MS sin enfermedades hematológicas asociadas.35 Dos de estos sujetos presentaron una mejoría sintomática inicial, pero luego evolucionaron con LMA y fallecieron. En un estudio diferente, se observó optimización de los síntomas en un individuo con MS-NHNM tratado con dasatinib.36 En otro ensayo, un enfermo con MSA falleció rápidamente a pesar de la terapia con cladribina y dasatinib.37 Nuestro paciente fue el caso con mejor respuesta al tratamiento con dasatinib (en combinación con la quimioterapia) mencionado en la bibliografía.15 La LMA de este enfermo ha permanecido en remisión hematológica completa por más de 42 meses. Desde el punto de vista morfológico, el recuento de mastocitos disminuyó significativamente. Se hace énfasis en que se logró una remisión molecular (la mutación KITD816V se convirtió en indetectable). La remisión molecular se ha preservado con la terapia de mantenimiento con dasatinib en este paciente. Este resultado indica que no todos los mastocitos neoplásicos contienen la mutación KITD816V o, en otros términos, los mastocitos son heterogéneos y, a diferencia de lo señalado en la LMC, la supervivencia de los mastocitos neoplásicos depende de más de una aberración genética.
La midostaurina (PKC412) aparece como el ITQ más promisorio para el tratamiento de la MS. En un estudio de fase II, Gotlib y col. demostraron que la administración de 100 mg de midostaurina 2 veces al día se asoció con una respuesta global del 73% en 15 pacientes con MSA (cinco de ellos con respuesta mayor y otros seis con respuesta parcial).38 El nilotinib fue activo contra los mastocitos con c-KIT natural o aquellos con la mutación yuxtamembrana D560G de este gen, pero no lo fue en aquellos mastocitos que expresaban la tirosina quinasa con la mutación KITD816V.39 En un estudio de fase II se evaluó el uso de 400 mg de nilotinib 2 veces al día en 60 pacientes con MS.40 La mutación KITD816V fue positiva en el 83% de los 36 enfermos en los cuales se estudió su presencia. La respuesta global sólo se confirmó en doce de esos sujetos (20%).
Se considera importante determinar la respuesta a los ITQ en pacientes con MS-NHNM. En algunos informes se señaló que las células hematológicas malignas asociadas presentan la misma mutación en el gen KIT.15,41-45 Este hallazgo permite avalar el concepto de un progenitor neoplásico común para los mastocitos neoplásicos y las células hematológicas malignas. En consecuencia, tanto la MS como la neoplasia hematológica podrían mejorar con el uso de ITQ en los sujetos con MS-NHNM.
En nuestro paciente, la combinación de dasatinib y quimioterapia provocó la eliminación de los mieloblastos y los mastocitos neoplásicos portadores de la mutación KITD816V. Consideramos que el dasatinib mejoró la evolución de este enfermo en el contexto de una afección que se caracteriza por un muy mal pronóstico.
Los autores no manifiestan conflictos de intereses.
Molecular and Clinical Efficacy of Dasatinib in Systemic Mastocytosis Associated with Acute Myelogenous Leukemia
(especial para SIIC © Derechos reservados)
(especial para SIIC © Derechos reservados)
Introduction
Systemic mastocytosis (SM), a clonal neoplastic proliferation of mast cells, is defined as mast cell infiltration of at least one extracutaneous organ with or without evidence of skin involvement by the World Health Organization (WHO).1 SM is a very heterogeneous disorder, including indolent forms such as indolent SM with a normal life expectancy.1,2 SM has also aggressive forms, including aggressive SM (ASM), mast cell sarcoma, and mast cell leukemia.1,2 SM with an associated clonal hematological non-mast cell lineage disease (SM-AHNMD) accounts for 20-30% of SM.1,2 The prognosis of SM-AHNMD depends mostly on the prognosis of concurrent hematologic malignancy. Almost all hematologic malignancies except for Hodgkin’s disease were reported as an associated hematologic malignancy in SM-AHNMD.3-8 The most frequently associated malignancies are myelogenous such as acute myelogenous leukemia (AML), chronic myelomonocytic leukemia (CMML), and chronic myeloid leukemia (CML).3 Recently, two concurrent hematologic malignancies were reported in a patient with SM.9 More than 90% of patients with SM contain an activating point mutation within KIT. This class III receptor tyrosine kinase consists of an extracellular domain with five immunoglobulin-like repeats, a single transmembrane domain, a juxtamembrane domain, and a cytoplasmic tyrosine kinase domain.10 The most common point mutation, KITD816V, resulted from substitution of valin for asparaginase at codon 816 within KIT exon 17.11 Because of ligand-independent activation of the KIT tyrosine kinase, imatinib, a tyrosine kinase inhibitor (TKI), standard treatment for chronic myeloid leukemia (CML), is often used in SM.11-13 However, it was found to be ineffective.11-13 Dasatinib, a second line TKI for treatment of CML, was also used in patients with SM.14-15 We published a case report in which dasatinib with chemotherapy provided long-term survival.15 More interestingly, the KITD816V mutation became undetectable after treatment (the full case report is available in the journal Leukemia Research). Herein, we give a summary of treatment and an update on the patient.
Case report
A 51-year-old male presented with a history of fatigue, abdominal pain, and weight loss in January 2007. A bone marrow (BM) aspirate/biopsy was performed because of the presence of blasts in the peripheral blood (PB). Two distinct cell populations were detected: 1) myeloblasts (positive for HLA-DR, CD34, CD13) and 2) round or spindle shaped mast cells (positive for CD25, CD117, CD64, HLA-DR, CD13, CD33, CD36, MPO, CD11c and negative for CD34). Cytogenetic and molecular studies revealed normal karyotype. Bidirectional sequencing of KIT exon 17 demonstrated a D816V mutation in the diagnostic BM sample. A CT scan of the abdomen and pelvis revealed hepatosplenomegaly, lymphadenopathy, and lytic bone lesions in the pelvis. The patient was diagnosed with SM-AHNMD (SM + AML). SM diagnosis was made by the presence of one major (i.e., > 15 mast cells aggregating in the BM) and four minor WHO criteria (i.e., spindling morphology, CD25 positivity, the presence of KITD816V mutation, and elevated serum tryptase). The patient achieved a complete hematologic remission (CHR) with reinduction in terms of AML. Mast cells were retained in the remission BM. The patient continued consolidation therapy with high dose cytarabine because alloHSCT was not available for him. Dasatinib (Sprycel®, obtained from the patient support program of Bristol-Myers Squibb as a courtesy) was added to consolidation therapy at a dose of 70 mg twice a day. Dasatinib has been continued as maintenance therapy to date. Because of mild to moderate cytopenias, its dose was reduced to 50 mg/d. Morphologically, the patient remained in CHR in terms of AML, and partial response (PR) in terms of SM. Lytic bone lesions were slightly improved as shown by repeated CT scans. The KITD816V mutation became undetectable (Table 1). The last BM biopsy (1 year after publication) confirmed the same results (Table 1). Recently, a liver biopsy on the patient performed for the elevation of liver enzymes showed mast cells infiltration and stage II/III periportal fibrosis. We were able to do in vitro analyses on the patients’ primary CD34+ (including myeloblasts) and CD34- cells (including mast cells). Both the CD34+ cells and CD34- cells were found to be positive for the KITD816V mutation at the time of diagnosis but became negative after treatment. The c-KIT mutation analyses were done by two different independent laboratories and were consistent. In addition, dasatinib treatment diminished the activity of STAT5, STAT3, AKT and ERK, attenuated the levels of c-KIT in CD34-cells and induced loss of viability in CD34- cells.
Discussion
The prognosis of ASM patients is poor, and these patients require “cytoreductive therapy”.1,2 Interferon-? and cladribine are the most commonly used cytoreductive drugs,1,2 but overall response (OR) rate has been around 50% to 60% with lower CR rates with these medications.1,2,16 TKIs have become an attractive option because there is no standard therapy for patients with ASM. The first TKI used in SM was imatinib. Imatinib is effective in vitro or in vivo in SM with no mutation or with certain mutations like PDGFR. However, imatinib is inactive if the KITD816V mutation exists.17-34 Its inefficacy in the presence of the KITD816V mutation is attributed to the changed conformation of the activation loop lying at the entrance to the KIT enzymatic pocket which interferes with the binding of imatinib.17-20 In a phase II trial, 20 patients received imatinib (400 mg daily) with a median of 9 months.24 Only one patient (SM with hypereosinophilic syndrome without the KITD816V mutation) achieved CHR whereas 6 patients showed symptomatic improvement and 13 patients had no response. An Italian group retrospectively analyzed 24 advanced SM patients. Imatinib was the most common drug used in these patients (29%).25 In these, the response rate was low (one CHR and four PR). More interestingly, all responsive patients had no evidence of the KITD816V mutation. In a different study Pardanini et al showed that out of 10 patients, OR was demonstrated in 5 patients. All responsive patients were negative for the KITD816V mutation.26 In contrast to these studies, one phase II trial found imatinib clinically effective (i.e., reduction in > 2 endpoints per their description of efficacy in the study) in all patients with the KITD816V mutation positivity.27 End points evaluated were serum tryptase, urinary N-methylhistamine excretion, skin lesions, the number of mast cells in bone marrow sections, hepatomegaly and/or splenomegaly, and symptoms.27 In this case, imatinib was administered at a dose of 400 mg once daily for 3 to 6 months in 14 patients. Eleven of these patients had the KITD816V mutation. Many results in the literature on dasatinib use with patients with SM have been relatively poor. One study in which dasatinib was evaluated in a phase II trial produced OR in 30% of 33 SM patients (18 indolent, 9 aggressive, and 6 with associated hematologic malignancy).14 Out of the six patients with associated hematologic malignancy, three initially showed a major response to dasatinib, but the majority (4/6) died (one due to progression to AML). Of the two SM-AHNMD patients (one with myelofibrosis – MF –and the other one with hypereosinophilic syndrome) who achieved a CHR, neither was KITD816V mutation positive. The SM-MF patient later progressed to AML and died. In another study, 4 SM patients with no associated hematologic malignancy received dasatinib.35 Two had symptomatic improvement initially but then progressed to AML and died. In a separate study, a patient with SM-CMML receiving dasatinib achieved symptomatic improvement.36 In a different study another patient with ASM died quickly despite cladribine and dasatinib treatment.37 Our patient may be the most successfully treated patient with dasatinib (in a combination with chemotherapy) in the literature.15 The patient’s AML has been in CHR for more than 42 months. Morphologically, mast cell counts decreased significantly. More importantly, the patient achieved a molecular remission (i.e, the KITD816V mutation became undetectable). Molecular remission has been durable on dasatinib maintenance in the patient. This indicates that not all neoplastic mast cells contain the KITD816V mutation or in other words, mast cells are heterogeneous, and unlike in CML, the survival of neoplastic mast cells depends on more than one genetic aberration.
Midostaurin (PKC412) appears to be the most promising TKI in SM. In a phase II trial, Gotlib et al showed midostaurin 100 mg twice a day resulted in an OR in 73% of 15 ASM patients (5 with major response and 6 with PR).38 Nilotinib was active in wild type c-KIT mast cells or those harboring the juxtamembrane D560G c-kit mutant, but not in mast cells expressing the KITD816V mutant tyrosine kinase.39 A phase II trial evaluated nilotinib (400 mg twice a day) in 60 patients with SM.40 The KITD816V mutation was positive in 83% of the 36 patients tested. OR was observed in only 12 of these patients (20%). It would be interesting to evaluate responses to TKIs in patients with SM-AHNMD. In some reports, there is evidence that associated hematologic malignant cells have the same KIT mutation.15,41-45 This finding supports the notion that there is a common neoplastic progenitor from which malignant mast cells and hematologic malignancy rise. Therefore, SM as well as hematologic malignancy may improve by using TKIs in SM-AHNMD. In our patient, dasatinib in combination with chemotherapy resulted in the clearance of the KITD816V mutation positive mast cells and myeloblasts. We believe that dasatinib improved the outcome of this patient in the face of a very poor prognostic disease.
Systemic mastocytosis (SM), a clonal neoplastic proliferation of mast cells, is defined as mast cell infiltration of at least one extracutaneous organ with or without evidence of skin involvement by the World Health Organization (WHO).1 SM is a very heterogeneous disorder, including indolent forms such as indolent SM with a normal life expectancy.1,2 SM has also aggressive forms, including aggressive SM (ASM), mast cell sarcoma, and mast cell leukemia.1,2 SM with an associated clonal hematological non-mast cell lineage disease (SM-AHNMD) accounts for 20-30% of SM.1,2 The prognosis of SM-AHNMD depends mostly on the prognosis of concurrent hematologic malignancy. Almost all hematologic malignancies except for Hodgkin’s disease were reported as an associated hematologic malignancy in SM-AHNMD.3-8 The most frequently associated malignancies are myelogenous such as acute myelogenous leukemia (AML), chronic myelomonocytic leukemia (CMML), and chronic myeloid leukemia (CML).3 Recently, two concurrent hematologic malignancies were reported in a patient with SM.9 More than 90% of patients with SM contain an activating point mutation within KIT. This class III receptor tyrosine kinase consists of an extracellular domain with five immunoglobulin-like repeats, a single transmembrane domain, a juxtamembrane domain, and a cytoplasmic tyrosine kinase domain.10 The most common point mutation, KITD816V, resulted from substitution of valin for asparaginase at codon 816 within KIT exon 17.11 Because of ligand-independent activation of the KIT tyrosine kinase, imatinib, a tyrosine kinase inhibitor (TKI), standard treatment for chronic myeloid leukemia (CML), is often used in SM.11-13 However, it was found to be ineffective.11-13 Dasatinib, a second line TKI for treatment of CML, was also used in patients with SM.14-15 We published a case report in which dasatinib with chemotherapy provided long-term survival.15 More interestingly, the KITD816V mutation became undetectable after treatment (the full case report is available in the journal Leukemia Research). Herein, we give a summary of treatment and an update on the patient.
Case report
A 51-year-old male presented with a history of fatigue, abdominal pain, and weight loss in January 2007. A bone marrow (BM) aspirate/biopsy was performed because of the presence of blasts in the peripheral blood (PB). Two distinct cell populations were detected: 1) myeloblasts (positive for HLA-DR, CD34, CD13) and 2) round or spindle shaped mast cells (positive for CD25, CD117, CD64, HLA-DR, CD13, CD33, CD36, MPO, CD11c and negative for CD34). Cytogenetic and molecular studies revealed normal karyotype. Bidirectional sequencing of KIT exon 17 demonstrated a D816V mutation in the diagnostic BM sample. A CT scan of the abdomen and pelvis revealed hepatosplenomegaly, lymphadenopathy, and lytic bone lesions in the pelvis. The patient was diagnosed with SM-AHNMD (SM + AML). SM diagnosis was made by the presence of one major (i.e., > 15 mast cells aggregating in the BM) and four minor WHO criteria (i.e., spindling morphology, CD25 positivity, the presence of KITD816V mutation, and elevated serum tryptase). The patient achieved a complete hematologic remission (CHR) with reinduction in terms of AML. Mast cells were retained in the remission BM. The patient continued consolidation therapy with high dose cytarabine because alloHSCT was not available for him. Dasatinib (Sprycel®, obtained from the patient support program of Bristol-Myers Squibb as a courtesy) was added to consolidation therapy at a dose of 70 mg twice a day. Dasatinib has been continued as maintenance therapy to date. Because of mild to moderate cytopenias, its dose was reduced to 50 mg/d. Morphologically, the patient remained in CHR in terms of AML, and partial response (PR) in terms of SM. Lytic bone lesions were slightly improved as shown by repeated CT scans. The KITD816V mutation became undetectable (Table 1). The last BM biopsy (1 year after publication) confirmed the same results (Table 1). Recently, a liver biopsy on the patient performed for the elevation of liver enzymes showed mast cells infiltration and stage II/III periportal fibrosis. We were able to do in vitro analyses on the patients’ primary CD34+ (including myeloblasts) and CD34- cells (including mast cells). Both the CD34+ cells and CD34- cells were found to be positive for the KITD816V mutation at the time of diagnosis but became negative after treatment. The c-KIT mutation analyses were done by two different independent laboratories and were consistent. In addition, dasatinib treatment diminished the activity of STAT5, STAT3, AKT and ERK, attenuated the levels of c-KIT in CD34-cells and induced loss of viability in CD34- cells.
Discussion
The prognosis of ASM patients is poor, and these patients require “cytoreductive therapy”.1,2 Interferon-? and cladribine are the most commonly used cytoreductive drugs,1,2 but overall response (OR) rate has been around 50% to 60% with lower CR rates with these medications.1,2,16 TKIs have become an attractive option because there is no standard therapy for patients with ASM. The first TKI used in SM was imatinib. Imatinib is effective in vitro or in vivo in SM with no mutation or with certain mutations like PDGFR. However, imatinib is inactive if the KITD816V mutation exists.17-34 Its inefficacy in the presence of the KITD816V mutation is attributed to the changed conformation of the activation loop lying at the entrance to the KIT enzymatic pocket which interferes with the binding of imatinib.17-20 In a phase II trial, 20 patients received imatinib (400 mg daily) with a median of 9 months.24 Only one patient (SM with hypereosinophilic syndrome without the KITD816V mutation) achieved CHR whereas 6 patients showed symptomatic improvement and 13 patients had no response. An Italian group retrospectively analyzed 24 advanced SM patients. Imatinib was the most common drug used in these patients (29%).25 In these, the response rate was low (one CHR and four PR). More interestingly, all responsive patients had no evidence of the KITD816V mutation. In a different study Pardanini et al showed that out of 10 patients, OR was demonstrated in 5 patients. All responsive patients were negative for the KITD816V mutation.26 In contrast to these studies, one phase II trial found imatinib clinically effective (i.e., reduction in > 2 endpoints per their description of efficacy in the study) in all patients with the KITD816V mutation positivity.27 End points evaluated were serum tryptase, urinary N-methylhistamine excretion, skin lesions, the number of mast cells in bone marrow sections, hepatomegaly and/or splenomegaly, and symptoms.27 In this case, imatinib was administered at a dose of 400 mg once daily for 3 to 6 months in 14 patients. Eleven of these patients had the KITD816V mutation. Many results in the literature on dasatinib use with patients with SM have been relatively poor. One study in which dasatinib was evaluated in a phase II trial produced OR in 30% of 33 SM patients (18 indolent, 9 aggressive, and 6 with associated hematologic malignancy).14 Out of the six patients with associated hematologic malignancy, three initially showed a major response to dasatinib, but the majority (4/6) died (one due to progression to AML). Of the two SM-AHNMD patients (one with myelofibrosis – MF –and the other one with hypereosinophilic syndrome) who achieved a CHR, neither was KITD816V mutation positive. The SM-MF patient later progressed to AML and died. In another study, 4 SM patients with no associated hematologic malignancy received dasatinib.35 Two had symptomatic improvement initially but then progressed to AML and died. In a separate study, a patient with SM-CMML receiving dasatinib achieved symptomatic improvement.36 In a different study another patient with ASM died quickly despite cladribine and dasatinib treatment.37 Our patient may be the most successfully treated patient with dasatinib (in a combination with chemotherapy) in the literature.15 The patient’s AML has been in CHR for more than 42 months. Morphologically, mast cell counts decreased significantly. More importantly, the patient achieved a molecular remission (i.e, the KITD816V mutation became undetectable). Molecular remission has been durable on dasatinib maintenance in the patient. This indicates that not all neoplastic mast cells contain the KITD816V mutation or in other words, mast cells are heterogeneous, and unlike in CML, the survival of neoplastic mast cells depends on more than one genetic aberration.
Midostaurin (PKC412) appears to be the most promising TKI in SM. In a phase II trial, Gotlib et al showed midostaurin 100 mg twice a day resulted in an OR in 73% of 15 ASM patients (5 with major response and 6 with PR).38 Nilotinib was active in wild type c-KIT mast cells or those harboring the juxtamembrane D560G c-kit mutant, but not in mast cells expressing the KITD816V mutant tyrosine kinase.39 A phase II trial evaluated nilotinib (400 mg twice a day) in 60 patients with SM.40 The KITD816V mutation was positive in 83% of the 36 patients tested. OR was observed in only 12 of these patients (20%). It would be interesting to evaluate responses to TKIs in patients with SM-AHNMD. In some reports, there is evidence that associated hematologic malignant cells have the same KIT mutation.15,41-45 This finding supports the notion that there is a common neoplastic progenitor from which malignant mast cells and hematologic malignancy rise. Therefore, SM as well as hematologic malignancy may improve by using TKIs in SM-AHNMD. In our patient, dasatinib in combination with chemotherapy resulted in the clearance of the KITD816V mutation positive mast cells and myeloblasts. We believe that dasatinib improved the outcome of this patient in the face of a very poor prognostic disease.
Celalettin Ustun, University of Minnesota Department of Medicine Section of Hematology Oncology and Transplantation, MN55455, Mineápolis, EE.UU.,
e-mail: custun@mail.mcg.edu
1. Horny HP, Akin C, Metcalfe DD, et al. Mastocytosis (Mast cell disease). In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, eds. World Health Organization (WHO) Classification of Tumours. Pathology & Genetics. Tumours of Haematopoietic and Lymphoid Tissues, IARC Press: Lyon, France. vol 2. pp. 54-63, 2008.
2. Lim KH, Tefferi A, Lasho TL, Finke C, Patnaik M, Butterfield JH, McClure RF, Li CY, Pardanani A. Systemic mastocytosis in 342 consecutive adults: survival studies and prognostic factors. Blood 113:5727-36, 2009.
3. Sperr WR, Horny H-P, Lechner K, et al. Clinical and biologic diversity of leukemias occurring in patients with mastocytosis. Leuk Lymphoma 37:473-86, 2000.
4. Sperr WR, Horny HP, Valent P. Spectrum of associated clonal hematologic nonmast cell lineage disorders occurring in patients with systemic mastocytosis. Int Arch Allergy Immunol 127:140-2, 2002.
5. Pullarkat ST, Sedarat F, Paquette R, et al. Systemic mastocytosis with plasma cell dyscrasia: report of a case. Leuk Res 32:1160-3, 2008.
6. Horny H-P, Sotlar K, Stellmacher F, et al. An unusual case of systemic mastocytosis associated with chronic lymphocytic leukaemia (SM-CLL). J Clin Pathol 59:264-8, 2006.
7. Tzankov A, Sotlar K, Muhlematter D, et al. Systemic mastocytosis with associated myeloproliferative disease and precursor B lymphoblastic leukaemia with t(13;13)(q12;q22) involving FLT3. J Clin Pathol 61:958-61, 2008.
8. Pullarkat VA, Bueso-Ramos C, Lai R, et al. Systemic mastocytosis with associated clonal hematological non-mast-cell lineage disease: analysis of clinicopathologic features and activating c-kit mutations. Am J Hematol 73:12-7, 2003.
9. Du S, Rashidi HH, Le DT, Kipps TJ, et al. Systemic mastocytosis in association with chronic lymphocytic leukemia and plasma cell myeloma. Int J Clin Exp Pathol 3:448-57, 2010.
10. Nagata H, Worobec AS, Oh CK, et al. Identification of a point mutation in the catalytic domain of the protooncogene c-KIT in peripheral blood mononuclear cells of patients who have mastocytosis with an associated hematologic disorder. Proc Natl Acad Sci USA 92:10560-4, 1995.
11. Hungness SI, Akin C. Mastocytosis: advances in diagnosis and treatment. Curr Allergy Asthma Rep 7:248-54, 2007.
12. Frost MJ, Ferrao PT, Hughes TP, Ashman LK. Juxtamembrane mutant V560GKit is more sensitive to Imatinib (STI571) compared with wild-type c-KIT whereas the kinase domain mutant D816VKit is resistant. Mol Cancer Ther 1:1115-24, 2002.
13. Foster R, Griffith R, Ferrao P, Ashman L. Molecular basis of the constitutive activity and STI571 resistance of Asp816Val mutant KIT receptor tyrosine kinase. J Mol Graph Model 23:139-52, 2004.
14. Verstovsek S, Tefferi A, Cortes J, et al. Phase II study of dasatinib in Philadelphia chromosome-negative acute and chronic myeloid diseases, including systemic mastocytosis. Clin Cancer Res 14:3906-15, 2008.
15. Ustun C, Corless CL, Savage N, et al. Chemotherapy and dasatinib induce long-term hematologic and molecular remission in systemic mastocytosis with acute myeloid leukemia with KIT D816V. Leuk Res 33:735-41, 2009.
16. Lim KH, Pardanani A, Butterfield JH, et al. Cytoreductive therapy in 108 adults with systemic mastocytosis: Outcome analysis and response prediction during treatment with interferon-alpha, hydroxyurea, imatinib mesylate or 2-chlorodeoxyadenosine. Am J Hematol 84:790-4, 2009.
17. Akin C, Brockow K, D'Ambrosio C, et al. Effects of tyrosine kinase inhibitor STI571 on human mast cells bearing wild-type or mutated c-kit. Exp Hematol 31:686-92, 2003.
18. Frost MJ, Ferrao PT, Hughes TP, Ashman LK. Juxtamembrane mutant V560GKit is more sensitive to Imatinib (STI571) compared with wild-type c-kit whereas the kinase domain mutant D816VKit is resistant. Mol Cancer Ther 1:1115-24, 2002.
19. Ma Y, Zeng S, Metcalfe DD, et al. The c-KIT mutation causing human mastocytosis is resistant to STI571 and other KIT kinase inhibitors; kinases with enzymatic site mutations show different inhibitor sensitivity profiles than wild-type kinases and those with regulatory-type mutations. Blood 99:1741-4, 2002.
20. Zermati Y, De Sepulveda P, Féger F, et al. Effect of tyrosine kinase inhibitor STI571 on the kinase activity of wild-type and various mutated c-kit receptors found in mast cell neoplasms. Oncogene 22:660-4, 2003.
21. Heinrich MC, Griffith DJ, Druker BJ, et al. Inhibition of c-kit receptor tyrosine kinase activity by STI 571, a selective tyrosine kinase inhibitor. Blood 96:925-32, 2000.
22. Yamada Y, Cancelas JA. FIP1L1/PDGFR alpha-associated systemic mastocytosis. Int Arch Allergy Immunol 152(Suppl.1):101-5, 2010.
23. Lahortiga I, Akin C, Cools J, et al. Activity of imatinib in systemic mastocytosis with chronic basophilic leukemia and a PRKG2-PDGFRB fusion. Haematologica 93:49-56, 2008.
24. Vega-Ruiz A, Cortes JE, Sever M, et al. Phase II study of imatinib mesylate as therapy for patients with systemic mastocytosis. Leuk Res 33(11):1481-4, 2009.
25. Pagano L, Valentini CG, Caira M, et al Advanced mast cell disease: an Italian Hematological Multicenter experience. Int J Hematol 88:483-8, 2008.
26. Pardanani A, Elliott M, Reeder T, et al. Imatinib for systemic mast-cell disease. Lancet 362:535-6, 2003.
27. Droogendijk HJ, Kluin-Nelemans HJ, et al.Imatinib mesylate in the treatment of systemic mastocytosis: a phase II trial. Cancer 107:345-51, 2006.
28. Florian S, Esterbauer H, Binder T, et al. Systemic mastocytosis (SM) associated with chronic eosinophilic leukemia (SM-CEL): detection of FIP1L1/PDGFRalpha, classification by WHO criteria, and response to therapy with imatinib. Leuk Res 30:1201-5, 2006.
29. Hoffmann KM, Moser A, Lohse P, et al. Successful treatment of progressive cutaneous mastocytosis with imatinib in a 2-year-old boy carrying a somatic KIT mutation. Blood 112:1655-7, 2008.
30. Akin C, Fumo G, Yavuz AS, et al. A novel form of mastocytosis associated with a transmembrane c-kit mutation and response to imatinib. Blood 103:3222-5, 2004.
31. Pardanani A, Verstovsek S. Hypereosinophilic syndrome, chronic eosinophilic leukemia, and mast cell disease. Cancer J 13:384-91, 2007.
32. Zhang LY, Smith ML, Schultheis B, et al.A novel K509I mutation of KIT identified in familial mastocytosis-in vitro and in vivo responsiveness to imatinib therapy. Leuk Res 30:373-8, 2006.
33. Pardanani A, Ketterling RP, Brockman SR, et al. CHIC2 deletion, a surrogate for FIP1L1-PDGFRA fusion, occurs in systemic mastocytosis associated with eosinophilia and predicts response to Imatinib therapy. Blood 2003.
34. Heinrich MC, Joensuu H, Demetri GD, et al. Imatinib Target Exploration Consortium Study B2225. Phase II, open-label study evaluating the activity of imatinib in treating life-threatening malignancies known to be associated with imatinib-sensitive tyrosine kinases. Clin Cancer Res 14:2717-25, 2008.
35. Purtill D, Sinniah R, Cooney J, et al. Dasatinib therapy for systemic mastocytosis: four cases. Eur J Haem 80:456-8, 2008.
36. Benz R, Boesiger J, Fehr J. Systemic mastocytosis with c-KITD816V mutation treated with dasatinib. Blood 110:258b, 2007.
37. Aichberger KJ, Sperr WR, Gleixner KV, et al. Treatment responses to cladribine and dasatinib in rapidly progressing aggressive mastocytosis. Eur J Clin Invest 38:869-73, 2008.
38. Gotlib J, George TI, Corless C, et al. The KIT tyrosine kinase inhibitor midostaurine (PKC412) exhibits a high response rate in aggressive systemic mastocytosis (ASM): Interim results of a phase ii trial. Blood 110:3536, 2007.
39. Verstovsek S, Akin C, Manshouri T, et al. Effects of AMN107, a novel aminopyrimidine tyrosine kinase inhibitor, on human mast cells bearing wild-type or mutated codon 816 c-kit. Leuk Res 30:1365-70, 2006.
40. Hochhaus A, Ottmann OG, Lauber S, Hughes T, Verhoef G, Schwarer AP, Gratwohl A, Rafferty T, Resta D, Gattermann N.A phase II study of nilotinib, a novel inhibitor of c-Kit, PDGFR, and Bcr-Abl, administered to patients with systemic mastocytosis. Blood 108:2703, 2006.
41. Yavuz A, Lipsky PE, Yavuz S, et al. Evidence for the involvement of a hematopoietic progenitor cell in systemic mastocytosis from single-cell analysis of mutations in the c-kit gene. Blood 100:661-665, 2002
42. Akin C, Kirshenbaum AS, Semere T, et al. Analysis of the surface expression of c-kit and occurrence of the c-kit Asp816Val activating mutation in T cells, B cells, and myelomonocytic cells in patients with mastocytosis. Exp Hematol 28:140-147, 2000.
43. Nagai S, Ichikawa M, Takahashi T, et al. The origin of neoplastic mast cells in systemic mastocytosis with AML1/ETO-positive acute myeloid leukemia Exp Hematol 35:1747-52, 2007.
44. Pullarkat V, Bedell V, Kim Y, et al. Neoplastic mast cells in systemic mastocytosis associated with t(8;21) acute myeloid leukemia are derived from the leukemic clone. Leuk Res 31:261-5, 2007.
45. McClintock-Treep SA, Horny HP, Sotlar K, Foucar MK, Reichard KK. KIT(D816V+) systemic mastocytosis associated with KIT(D816V+) acute erythroid leukaemia: first case report with molecular evidence for same progenitor cell derivation. J Clin Pathol 62:1147-9, 2009.
Artículos publicados por el autor
(selección)
Wang Y, Fiskus W, Chong DG, Buckley KM, Natarajan K, Rao R, Joshi A, Koul S, Chen J, Savoie A, Ustun C, Jillella A, Levine RL, Bhalla K. Co-treatment with panobinostat and JAK2 inhibitor TG101209 attenuates JAK2-V617F levels and signaling and exerts synergistic cytotoxic effects against human myeloproliferative neoplasm cells Blood 114(114):33-33, 2009
Tanna Saloni, Ustun C. Immunosuppressive treatment in patient with pure red cell aplasia associated with chronic myelomonocytic leukemia; harm or benefit? International Journal of Hematology 90:597-600, 2009
Ustun C, Deremer D, Jillella A, Bhalla K. Investigational drugs targeting flt3 for leukemia Expert Opinion on Investigational Drugs 18:1445-1456, 2009
Fiskus W, Wang Y, Sreekumar A, Buckley K, Shi H, Jillella A, Ustun C, et al. Combined epigenetic therapy with the histone methyltransferase EZH2 inhibitor 3-deazaneplanocin A and the histone deacetylase inhibitor panobinostat against human AML cells Blood 114:2733-2743, 2009
Subbannan K, Ustun C, Natarajan K, et al. Spleen related complications and implications of splenectomy in patients with hemoglobin SC disease International Journal of Hematology 83:258-260, 2009
Ustun C, Corless CL, Savage N, Fiskus W, Manaloor E, Heinrich MC, Lewis G, Ramalingam P, Kepten I, Jillella A, Bhalla K. Chemotherapy and dasatinib induce long-term hematologic and molecular remission in systemic mastocytosis with acute myeloid leukemia with KIT(D816V) Leukemia Research 33:735-741, 2009
Reid-Nicholson M, Nayak A, McDonald K, Crawford J, Jillella A, Ramalingham P. Plasmablastic lymphoma: CNS involvement, coexistence of other malignancies, possible viral etiology, and dismal outcome Annals of Hematology 88:351-358, 2009
Ustun C, Jillella AP, Salama ME. Dasatinib induces complete cytogenetic response and loss of F359C in an imatinib resistant chronic myelocytic leukemia patient American Journal of Hematology 84:386-387, 2009
Wang Y, Fiskus W, Chong DG, Buckley KM, Natarajan K, Rao R, Joshi A, Koul S, Chen J, Savoie A, Ustun C, Jillella A, Levine RL, Bhalla K. Co-treatment with panobinostat and JAK2 inhibitor TG101209 attenuates JAK2-V617F levels and signaling and exerts synergistic cytotoxic effects against human myeloproliferative neoplasm cells Blood 114(114):33-33, 2009
Tanna Saloni, Ustun C. Immunosuppressive treatment in patient with pure red cell aplasia associated with chronic myelomonocytic leukemia; harm or benefit? International Journal of Hematology 90:597-600, 2009
Ustun C, Deremer D, Jillella A, Bhalla K. Investigational drugs targeting flt3 for leukemia Expert Opinion on Investigational Drugs 18:1445-1456, 2009
Fiskus W, Wang Y, Sreekumar A, Buckley K, Shi H, Jillella A, Ustun C, et al. Combined epigenetic therapy with the histone methyltransferase EZH2 inhibitor 3-deazaneplanocin A and the histone deacetylase inhibitor panobinostat against human AML cells Blood 114:2733-2743, 2009
Subbannan K, Ustun C, Natarajan K, et al. Spleen related complications and implications of splenectomy in patients with hemoglobin SC disease International Journal of Hematology 83:258-260, 2009
Ustun C, Corless CL, Savage N, Fiskus W, Manaloor E, Heinrich MC, Lewis G, Ramalingam P, Kepten I, Jillella A, Bhalla K. Chemotherapy and dasatinib induce long-term hematologic and molecular remission in systemic mastocytosis with acute myeloid leukemia with KIT(D816V) Leukemia Research 33:735-741, 2009
Reid-Nicholson M, Nayak A, McDonald K, Crawford J, Jillella A, Ramalingham P. Plasmablastic lymphoma: CNS involvement, coexistence of other malignancies, possible viral etiology, and dismal outcome Annals of Hematology 88:351-358, 2009
Ustun C, Jillella AP, Salama ME. Dasatinib induces complete cytogenetic response and loss of F359C in an imatinib resistant chronic myelocytic leukemia patient American Journal of Hematology 84:386-387, 2009
Está expresamente prohibida la redistribución y la redifusión de todo o parte de los
contenidos de la Sociedad Iberoamericana de Información Científica (SIIC) S.A. sin
previo y expreso consentimiento de SIIC.
ua91218

